ContentslistsavailableatScienceDirect
Maturitas
j o ur na l h o me pa g e :w w w . e l s e v i e r . c o m / l o c a t e / m a t u r i t a s
Attitudes
and
perceptions
towards
vulvar
and
vaginal
atrophy
in
Italian
post-menopausal
women:
Evidence
from
the
European
REVIVE
survey
Rossella
E.
Nappi
a,∗,
Martire
Particco
b,
Nicoletta
Biglia
c,
Angelo
Cagnacci
d,
Costantino
Di
Carlo
e,
Stefano
Luisi
f,
Anna
Maria
Paoletti
gaResearchCenterforReproductiveMedicine,GynecologicalEndocrinologyandMenopause,IRCCSS.MatteoFoundation,DepartmentofClinical,Surgical,
DiagnosticandPaediatricSciences,UniversityofPavia,Pavia,Italy
bShionogiItaly,Rome,Italy
cDepartmentofObstetricsandGynaecology,UniversityofTorinoSchoolofMedicine,OspedaleMaurizianoUmbertoI,Torino,Italy dDepartmentofObstetricsandGynecology,UniversityofModena,Modena,Italy
eDepartmentofNeurosciencesandReproductiveSciences,UniversityofNaplesFedericoII,Naples,Italy
fObstetricsandGynecologyUnit,DepartmentofMolecularandDevelopmentalMedicine,UniversityofSiena,Siena,Italy gDepartmentofObstetricsandGynaecology,UniversityofCagliari,UniversityHospitalofCagliari,Cagliari,Italy
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received5April2016
Receivedinrevisedform31May2016 Accepted9June2016
Keywords:
Vulvarandvaginalatrophy Post-menopausalwomen REVIVEsurvey Sexualrelationships Vaginaldryness Dyspareunia
a
b
s
t
r
a
c
t
Objectives:ToachieveadeeperunderstandingoftheattitudesandperceptionsofItalianpost-menopausal
women(PMW)regardingvulvo-vaginalatrophy(VVA).
Studydesign:AspartoftheEUREVIVEstudy,anonlinesurveywasconductedinfourEuropeancountries;
theItalianarmcomprised1000participantsfromrepresentativeregionsofItaly.
Mainoutcomemeasures:Theperceptions,experiencesandneedsofItalianPMWinrelationtosexualand
vaginalhealth.
Results:ThemostfrequentVVAsymptomwasvaginaldryness(78%).Usually,theseverityofsymptoms
wassimilartoorworsethanwhentheyfirstappeared.Thiswasparticularlytruefordyspareunia,themost
bothersomesymptom(76%).VVAsymptomshadasignificantimpactonItalianparticipants’abilityto
achievepleasurablerelations(74%)andspontaneity(70%).Although75%ofparticipantswerestillsexually
active,theirsexdrivehadbeenreducedbyathirdbecauseofVVA.Womenexpectedthatdoctorswould
startadiscussionofmenopausalsymptomsandsexualhealth,butthiswasrarelythecase(11%).Most
womenhadbeentreatedwithavaginalover-the-counter(OTC)product.Womenwhohaddiscussed
theirconditionwithaphysicianweremorelikely(68%)tobeundertreatmentforVVAthanthosewho
hadnot(36%).Lowcompliancewasassociatedwithsymptomimprovement(23%),nothavingannoying
symptoms(22%),andtheimpossibilityifrestoringthevaginatonormal(14%).Commonreasonsfor
treatmentdissatisfactionwererelatedtorouteofadministrationordiscomfort.Lackofefficacyand
fearofahormoneeffectwereperceivedasthemainlimitationsforOTCandlocalestrogenproducts,
respectively.
Conclusions:DespitethecommonnessofVVAanditssignificantimpactonqualityoflife,thecondition
remainsunderdiagnosedinItaly.Discussionofsymptomswithdoctorsinfluencesthediagnosis,and
patients’satisfactionwithavailabletreatmentsisnothigh.
©2016TheAuthors.PublishedbyElsevierIrelandLtd.ThisisanopenaccessarticleundertheCC
BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:ResearchCentreforReproductiveMedicine,Section ofObstetricsandGynecology,IRCCSPoliclinicoSanMatteo,PiazzaleGolgi2,27100 Pavia,Italy.
E-mailaddress:renappi@tin.it(R.E.Nappi).
1. Introduction
Vulvarandvaginalatrophy(VVA),alsoknownasGenital Syn-dromeofMenopause(GSM)[1,2]afterarecentbroaderdefinition toincludeits globalimpactinuro-genital andsexualhealth, is achronicandprogressivepost-menopausalconditionassociated withthereductioninestrogenlevelsthatapproximatelyaffects 50%ofallpost-menopausalwomenworldwide[3–8].
http://dx.doi.org/10.1016/j.maturitas.2016.06.009
0378-5122/©2016TheAuthors.PublishedbyElsevierIrelandLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
R.E.Nappietal./Maturitas91(2016)74–80 75
TheVVAencompassesacomplexclusterofsymptomsthatmay varyaccordingtoage,durationofmenopause,frequencyof sex-ualintercourse,etc.Thepoorestrogenizationinuro-genitaland pelvictissuesmainlyresultsinvaginaldryness,irritation,lossof elasticity,decreasedlubrication,dyspareunia,andurinary symp-toms[3–8].PreviousEuropeanresearchhasshownthattheimpact ofVVAsymptomsinpost-menopausalwomenissignificant,since agrowingpercentageofthepopulationisagingandachievingtheir lastmenopauseperiod[9].Inadditiontoitsimpactonsexual func-tionandrelationshipwiththepartner,VVAcanhavesignificant influenceonmany dailyliving activitiesaswellas inwomen’s qualityoflife[2,10–12].
Asaconsequenceofthereportedpatient’sembarrassmentto askfor advice tohealthcare professionals (HCP) [10,12,13],the VVAclinicaldiagnosisandtreatmentisstillabridgeddespitethe highprevalenceand theconsiderableimpactoftheproblemin post-menopausal women [6,14].Thisunder-diagnosis turnsthe diseaseintoachronicandprogressiveconditioninmanycases[15]. Recently,differentcross-culturalsurveysontheimpactofVVAhave beenconductedonpost-menopausalwomen[14,16–21], suggest-ingthatVVAsymptomshaveasignificantglobalnegativeeffect onhealth,satisfaction,andsexualbehavior,despiteaccountingfor confoundingfactorsduetopopulationandculturalparticularities likethoseco-existinginEurope[22].
Theobjectiveofthepresentanalysis,basedontheREalWomen’s VIews of Treatment Options for Menopausal Vaginal ChangEs-Europe(REVIVE-EU)survey,wastoachieveadeeperunderstanding oftheVVAproblemknowledgebyItalianwomenaftermenopause, togetherwiththeirexperiencesandneedsintermsofsexualand vaginalhealth,aswellasthecurrentnatureoftheirinteractions withHCP.Thiswillhelp togain betterclinicaland therapeutic approaches,avoidingthemisconceptionsandspecificregretson estrogentherapythatusuallyjeopardizetheoptimizationofVVA management[6,23].
2. Methods
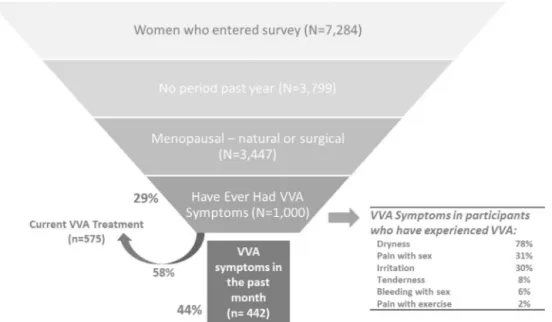
Followingthe same methodologyof the original US REVIVE survey, an online interview was conducted in several Euro-pean countries(Italy, Germany,Spain and United Kingdom)as describedpreviously[24].InItaly,ofatotalof7284women orig-inallyscreened,1000womenwithVVAsymptomswereincluded, beingdemographicallyrepresentativeofalltheItaliangeographic regions(North-East:19%,North-West:34%,Center:21%,South18%, Islands:8%).
The EUREVIVE survey wasoriginally translated and cultur-allyadaptedfromtheUSREVIVEversion(researchagency:Eikon Europe; panel used: Toluna Group), as well as pre-tested in a subsample of50 participantsbeforethebeginning ofthestudy period. The comprehensive online questionnaire was approved bythecorrespondingaccreditedinstitutional reviewboard.The surveyparticipantswereinformedof thestudyprocedures and gaveinformedconsenttoparticipate.TheEUREVIVEsurveylasted 35minandwasdesignedwithamarginerrorof3.1%atthe95% confidenceinterval.Theinvitationtoparticipatewassenttothe targetpopulation(post-menopausalwomenwithatleastoneVVA symptomaftertheonsetofmenopause)bythepanel(selectedby agerange).Participation wascompensatedwithpointsthatcan thenberedeemedforvouchersorgadgets(butnotforproducts ormoney).Participantsenteredthesecureonlinequestionnaire portalandcompletedthesurveybetweenmid-Juneandmid-July of 2014. Prior tothe completion of the questionnaire a three-stepscreeningprocesswascompleted(seeFig.1forthesedetails in the Italian participants). The information and variables col-lectedfromtheparticipantsincluded:knowledgeaboutVVAand
Table1
BaselinecharacteristicsoftheItaliansurveyedpopulation.
WomenreportingVVAsymptoms(n) 1000 Age(years),n(%) 45–50 99(9.9) 51–55 325(32.5) 56–60 309(30.9) 61–65 186(18.6) 66–70 60(6.0) 71–75 21(2.1) Maritalstatus,n(%) Married 673(67.3) Divorced 85(8.5) Domesticpartnership 71(7.1) Single 79(7.9) Widowed 52(5.2) Separated 40(4.0) Education/Employment,n(%) Employed 430(43.0)
Universityeducationorhighera 271(27.1)
Children,n(%) None 186(18.6) One 287(28.7) Two 386(38.6) Three 110(11.0) Fourormore 31(3.1) Childrenlivingathome,n(%) 544(67.0) PriortreatmentforVVAsymptoms,n(%) 787(79.0) OTCproduct 651(65.1) Prescriptionmedication 26(2.6) PrescriptionandOTCincombination 64(6.4) CurrenttreatmentforVVAsymptoms,n(%) 575(58.0) OTCproduct 492(49.2) Prescriptionmedication 28(2.8) PrescriptionandOTCincombination 1(0.01)
aIncludes:tradetraining,degreesandmaster’sdegrees;OTC:overthecounter.
menopausalsymptomatology,interactionswithHCPswithrespect toVVAsymptomatology,impactofVVAsymptomsonsexuallife anddailylivingactivities,currentorprevioususeofOTCproducts prescriptiontreatmentsforVVA,andpatient’sattitudestowards treatments.
Eligiblepatientswerethosewhofulfilledallselectioncriteria andwhohadvaliddatafortheconsideredvariables.Therewasno imputationofmissingdata.Theanalysisconsistedofadescriptive statisticsreportsummarizedbyrelativefrequencydistributionsfor categoricalvariablesofthesurvey.
3. Results
3.1. Populationdistribution
Thebaselinedemographicsand clinicalcharacteristicsof the finalsampleof1000ItalianparticipantsaresummarizedinTable1. The50–60agerangewasthemostrepresenteddemographicgroup inthesample(63%).Amongthecohortofparticipantssurveyed (Fig.1), 442(44%) had experienced VVAsymptomsin thepast month. At the beginning of the survey, 575(58%) of all those included participantswith VVAsymptoms were receiving VVA treatment.
3.2. VVAknowledgeandawareness
InItaly,withinthecohortofparticipantsthatwereawareof itsVVAcondition,thisknowledgeandinformationcamethrough activeinternetsearching(40%),newspaper/journalpaperreading (21%),talkswithfamilyorfriends(20%),anddirectdiscussionswith theirHCP/pharmacist(17%).Intheoverallsample,21%oftheItalian participantshadbeenclinicallydiagnosedwithVVAandformally
Fig.1. CharacteristicsoftheItaliansurveyedparticipants.
communicatedthatwaybyitsHCP,althoughthisratevaried geo-graphicallyreachingalmost30%inthecenterbutlessthan14%in thenortheastregion(2test,p<0.005).
3.3. VVAsymptomsandimpactonlife
ThemostfrequentsymptomoftheVVAconditioninsurveyed Italianpost-menopausalwomenatthemomentoftheinclusion wasvaginal dryness (78%), followed bydyspareunia (pain dur-ingintercourse)(31%),vaginalirritation(30%)andvaginal/vulvar tenderness(8%),withnosignificantdifferencesamongregions.A retrospectivesummaryof theonset of symptomsassociated or linkedwithVVAispresentedinFig.2.Mostparticipants(58%or more)reportedtheonsetofsymptomsduringthepost-menopausal period,althoughitvariedconsiderablyacrossmenopausestages dependingonthespecificsymptomatology.Vaginalirritationwas themostlikelysymptomtooccurbeforemenopause(16%),while vaginaldrynessandtendernesswerethemostlikelysymptomsto beginwithinthefirstyearaftermenstrualcessation(27%and26%, respectively).Theonsetofpainwithintercourseoccursacrossall themenopauseandpost-menopauseperiod,althoughitismost commonattheexactmomentofmenopause(28%)orduringthe subsequentyear(23%).
Themajorityofthecohortacknowledgedthatatthetime of thesurveytheseverityofsymptomswassimilarorworsethan whenit firstappeared(about 2/3ofcases),withparticular ref-erencetopainduringintercourse(75%),andwithoutdifferences amongcountryregions.Painassociatedwithsexwasratedasthe mostbothersomesymptom(76%participantssetitasbothersome orextremelybothersome),althoughallVVAsymptomswererated asquitebothersome.ParticipantsalsostatedthatVVAmadethem feelaging(45%),uncomfortable(37%),less feminine(16%), frus-trated(15%),worried(11%),anxious(11%) anddepressed(10%). ThemostconcerningfacetonmindreportedasaresultofVVA symptomswere“losingsexualintimacy”(47%)and“youth”(17%). ThehigherinterferenceofVVAsymptomswasacknowledgedby participantsonsexualsatisfaction(74%),followedbysexual spon-taneity(70%),intimacy(69%), andrelationshipwiththepartner (66%),respectively(Fig.3).
Italian participants who have a partner (81%) were cohab-itating in 85% of cases. The survey shows that 75% of Italian post-menopausalwomenwithVVAweresexuallyactiveduringthe
lastyear.Theanalysisshowedthatthestrengthofsexualdrivewas diminishedaround33%overall(2test,p<0.01)asadirectresult
ofVVAsymptomatology(30%inwomenwithpartnerand49%in womenwithoutpartner).
3.4. InteractionwithHCP
Overall,96%of participantsreportedvisitinga HCPfor their main gynecological needs (91% of them having a gynecolo-gist/obstetricianand17%ageneral/familypractitioner).Overhalf ofHCPswerefemalephysicians(54%).Duringthelastyear,71% oftheparticipantsconsultedtheirmainHCP,withthehigherrate inthesouth(76%)andthelowerintheislandsandthenorth-east region(68%,inbothcases).Only41%oftheparticipantswithan HCPforgynecologicalneedsacknowledgedthattheirHCPusually askedaboutthatparticipant’ssexualactivityduringroutine check-upvisits.TwothirdsofItalianparticipants(67%)haddiscussedVVA symptomswiththeirphysician.Italianwomeninislandswerethe participantswholessdiscusssymptomswiththeirHCP(60%)and thoseinthenorth-westtheoneswhodomore(71%).Threequarters (75%)ofparticipantsreportedthattheyexpecttheirHCPto specif-icallyaskaboutmenopause-relatedsymptoms,althoughonly11% ofthemsaidthattheHCPthemselveshadinitiatedthe conversa-tion(rangingbetween8%inthesouthand13%inthenorth-west region).
Themostcommonlyreportedreasonsfor neverdiscussVVA symptomswithHCPwerebeliefsthattheconditionwasa natu-ralpartoftheagingphenomenon(36%),followedbythestatement thatsymptomswerenotbothersomeenoughtowarrant discus-sion withtheirHCP (25%) and that theywill goaway in time (24%).Almost53%oftheparticipantshadreceivedadvice/support fromtheirpartneraboutVVAtreatment.Usually,dependingonthe specificsymptom,between62%(vaginal/vulvardryness)and76% (tenderness)ofparticipantsdiscussedtheproblemwithaHCP dur-ingthefirst6monthsexperiencingit.Italianparticipantsreported overallsatisfactionwithhowHCPhandledthefirstdiscussionabout VVAsymptoms(70%),thereceivedinformation(67%)andthe treat-mentoptionsproposedbythephysician(64%).
R.E.Nappietal./Maturitas91(2016)74–80 77
Fig.2. OnsetofVVAsymptomsinItalianwomencurrentlysufferingfromVVA.
Fig.3.VVAsymptominterferencewithsexuallifeandotheractivitiesinItaly.
3.5. ExperienceswithVVAtreatments
AmongthetotalItaliancohort,58%ofparticipantswere cur-rentlyusingaVVA-specifictreatment(Fig.4).Theoverallincidence ofwomennaïvetoanytreatmentwas21%(lowerinthenorththan inthesouthregions,2test,p<0.05)andanother21%hadlapsed
fromtheirtreatmentschedulewhenthesurveystarted.VVA treat-mentsweremainlyadministeredvaginallywithoutprescription (83%ofcurrentusers,mostlybenzocaineandcalendulaextract), whilevaginal prescriptiontherapies wereuncommon(3%), and an8%ofparticipantswereusingbothkindsofproducts(Fig.4). WomenwhohavediscussedtheirVVAsymptomswithanHCPwere morelikelytobeundercurrentmedication(68%vs.36%forthose whohadnotdiscussedsymptoms),aswellasthosewhohavebeen diagnosedfor VVA(94%vs. 75%).Participantsstarted theirVVA treatmentindifferentmanners:(1)23%throughaHCPprescription andtherecommendationofanOTCproducttobeusedtogether;
(2)15%startedusinganOTCproductthroughaHCPbefore receiv-ingspecificprescription;(3)12%begantreatmentthroughaHCP prescriptionwithoutpreciousOTCrecommendation;(4)another 12%startedusinganOTCproductbeforetalkingtoaHCP.
Anoverallratioof40%ofcurrentparticipantsabandonedtheir medicationatsomepointinthepast.Themostfrequentreasons forthislowcomplianceweretherelieffromVVAsymptoms(23%), notconsidersymptomsbothersomeenough(22%),thebeliefthat symptomswoulddiminishwithtime(15%),theinabilityof treat-menttoreverse thevaginal changes(14%) and thepriceof the product(13%).Inpatientswhocompletedorwerecurrentlytaking anOTCmedication,60%reportedoverallsatisfaction.Bycontrast, inpatientswhocompletedtheirlocalestrogenprescriptionorwho werecurrentlytakingit,51%showedglobalsatisfaction.
Italian participants also expressed their perception on VVA treatmentdifficulties(Table2).Usersof OTCmoisturizers were mainlyworriedabouttheimpossibilitytorestorethevaginainto
Fig.4. Participant’streatmentuse.
Table2
ViewsofVVAtherapiesinItalianparticipantscurrentlyusingtreatment.
OTCpersonalvaginalmoisturizer(n=333) OTCvaginallubricant(n=77) Prescriptionvaginalproduct(n=32) Issuesrelatedtorouteofadministration,n(%)
Messy 36(10.8) 8(10.4) 4(12.5)
Notdiscrete 12(3.6) 0(0.0) 1(3.1)
Notanoralpill 24(7.2) 3(3.9) 2(6.3)
Donotliketouchingbody 10(3.0) 1(1.3) 0(0.0)
Issuesrelatedtoconvenience,n(%)
Interruptsmydailyactivities/life 5(1.5) 1(1.3) 0(0.0)
Inconvenienttoadminister 26(7.8) 5(6.5) 6(18.8)
Cannotbesexuallyspontaneous 45(13.5) 5(6.5) 1(3.1)
Difficultdosingschedule 10(3.0) 2(2.6) 0(0.0)
Procedureofadministeringtreatment 13(3.9) 0(0.0) 2(6.3)
Issuesrelatedtosideeffects/safety,n(%)
Concernaboutbreastcancer 15(4.5) 1(1.3) 9(28.1)
Concernabouthormoneexposure 18(5.4) 2(2.6) 12(37.5)
Concernaboutlong-termusesafety 35(10.5) 8(10.4) 12(37.5)
Vaginaldischarge 21(6.3) 9(11.7) 4(12.5)
Concernaboutothersideeffects 30(9.0) 4(5.2) 11(34.4)
Experiencedsideeffects 7(2.1) 2(2.6) 1(3.1)
Partnerabsorbingestrogen 9(2.7) 1(1.3) 3(9.4)
Issuesrelatedtoefficacy,n(%)
Vaginanotrestoredtonaturalstate 86(25.8) 19(24.7) 10(31.3)
Notenoughreliefofsymptoms 36(10.8) 4(5.2) 1(3.1)
Takesalongtimetostartworking 25(7.5) 7(9.1) 3(6.3)
Other,n(%)
Expensive 38(11.4) 8(10.4) 1(3.1)
Negativeimpactonintimacy 12(3.6) 1(1.3) 1(3.1)
itsnormalconditions(25.8%),buttheyalsohadconcernsrelatedto
itsimpactonsexualspontaneity(13.5%),thepriceoftheproduct
(11.4%),thelimitationonsymptomrelief(10.8%)andthemessy
administration(10.8%).ParticipantsthatusedOTClubricantswere
mostlyworriedbythelimitationsoftheproductinrestoringthe
natural state of the vagina (24.7%), the side effects of vaginal
discharge(11.7%), itsmessiness(10.4%),itscost(10.4%)andthe
safetyofalong-termuse(10.4%).Finally,womenthatweretaking
VVAprescriptionproductsweremostworriedaboutsafetyissues
includingthelong-termsafety(37.5%),hormoneexposure(37.5%),
othersideeffects(34.4%)andbreastcancerrisks(28.1%),aswellas
withtheabilityoftheproducttorestorethevaginatoitsnatural
condition(31.3%).
4. Discussion
The post-hoc analysis of the Italian branch of 1000
post-menopausal women with recognizable VVA symptomatology
includedintheEuropeanversionoftheREVIVEstudy–thelargest
surveyofthisnaturetodate(n=3768)–highlightedthestill
sig-nificantlack of awareness of the VVAcondition bysubjects in
Italyandtheconsequencesforitseffectiveclinicaland
therapeu-tic management. A previousanalysis of theREVIVE survey has
detectedsignificantsocio-culturalbarriersinEuropefortheexact
VVAimpactinrelationwithpost-menopausalwomen’ssexual
sat-isfactionandspontaneity,aswellaswiththeirinteractionwith
HCP’s[22].Theseobservationstallyotherpreviousevidenceabout
thefactthatfemalesexualdysfunctionsoccuralongacontinuum fromdissatisfaction tocompletedysfunction linkedwith
socio-R.E.Nappietal./Maturitas91(2016)74–80 79
culturalfactorsthatmaymodulatetheexpressionandcomplaining modalities[20,25].Significantly,this healthvariationoccursnot onlyat acountrylevel, butalsoata regionallevel with signif-icantculturalorsocial differenceslikethose existingfor Italian regionsmorecentral-Europeandriveninthenorthandothersmore Mediterraneandriveninthesouth[26].
Aspreviouslyreportedinotherbackgrounds,theroleofvaginal drynessasoneofthemostsignificantVVAsymptomsassociated with menopause has been proved also here in Italian post-menopausalwomen[10,14,21,24].Symptomsgenerallyappeared earlyaftertheonsetofmenopauseandusuallydidnotresolveover time oreven worsened,even for Italianwomen that expressed higher treatmentsatisfaction than other Europeancountriesas evidencedbytheoverallEUREVIVEsurvey[21,24].Thefactthat only1/5ofthesurveyedwomeninItalywereformallydiagnosed withVVAandthatusuallytheylastformorethansixmonthsto discusssymptomswithaHCP,evidencedthatVVAisstill under-recognizedinthis country.Thisoccursinspiteofbeingdirectly associatedwithextremeburdenandwithprogressivebothersome symptomatologylikepainduringsexualintercourseandvaginal discomfortthatextremelycompromisessexualpleasureand spon-taneity[12,14,20,27].Thetrendtowardsanunderdiagnosewasalso depictedrecentlyinItalybytheAGATAstudygroupunderthemore wideperspectiveoftheGSMcondition[28].Infact,although
¾
of post-menopausalItalianwomeninoursurveyhaveacknowledged beingsexuallyactive,ourresultsshowedthat,afterVVA symp-tomsmanifestation,sexualdrivefalldownapercentageof30%in womenwithpartnerandalmosta50%inthosewithoutpartner. Thisobservationislikelyrelatedmainlywiththereductionof sex-ualsatisfactionthroughagingalsoreportedinItaly[29],aswell aswiththedemonstratedassociationofsexualfunctioninItalian womenwithoccurrenceofpainduringsexandwithsymptoms aftersexualintercourse[30].TheEuropeanREVIVEsurvey hasindicatedthat theeffective discussionofsymptoms andcommunicationwithanHCPhasa significantimpactbothontheincidenceofthediagnosisofVVA andthetherapeuticapproach.Thispatternhasbeenalsoobserved specificallyfortheItalianpost-menopausalwomen.Inthissense, thedatainItalyprovesthatwomenwhohaveconsulteda gyne-cologistdiscussmoreeasilyVVAandmenopausalsymptoms,and startsooneramedicaltreatment.Concretely,inthiscountry,among participantswhohavediscussedtheirVVAsymptomswith physi-cians,thepercentage ofwomenundertreatmentalmostdouble thatobservedonthosewhodidnotdiscusssymptoms. Further-more,although2/3ofItalianparticipantsacknowledgedthathave discussedVVAwiththeirHCP,theystillexpecttheirHCPto initi-ateproactivediscussiononsymptoms(75%),afactthatveryrarely happens(onlyoneintencases,asimilarratethanfortheoverallEU REVIVEsurvey).Despitetheseobservationsprovetheneedforan improvedawarenessbyHCPsregardingVVAanditsimpact,both thepercentageofwomenwhodiscusssymptomswithanHCPand thepercentageofsymptomaticparticipantsformallydiagnosedare higherforItalianpost-menopausalwomenthatfortheoverallEU REVIVEcohort[24].Thisisinagreementwithpreviousresultsof theCLOSERsurvey,whichalsoshowedsignificantlyhigher wor-riesinSouthernEuropeanpostmenopausalwomenwithlong-term vaginaldiscomfortanditsimpactontheirsexualrelationships[20]. Regardingthetherapeuticmanagementof VVAinItaly,VVA treatmentswereadministeredmainlyvaginallywithout prescrip-tion(OTC),althoughtheefficacyandsafetyofminimallyabsorbed localvaginalestrogenasVVAtherapyhasbeenextensivelyproven [31,32].ItalyisoneoftheEuropeancountriesstudiedwithhigher rateofcurrentuserssinceonly anoverall1/5ofItalian partici-pantsremainednaïvetoanytreatment(32%inEUREVIVE)and2/5 hasleftitatleastoncepreviously(23%inEUREVIVE).Main rea-sonsthatexplainwhywomenhavehadstillarelativelylowlevel
ofcompliancewithvaginaltreatmentsweretheresultofa com-plexspectrumofculturalelements(perceptionofimprovement andof notenoughannoyingsymptoms)and skepticalviewson thereversibilityofvaginalchanges[22].InItaly,effectivenesswas perceivedasthemainlimitationforOTCproductswhileforlocal estrogenwasthefearofhormoneeffect.Foralltherapeuticoptions themostfrequentreasonfordissatisfactionwasrelatedtotheroute ofadministrationordiscomfort[22].
Themainlimitationsofthisanalysisareadirectconsequence oftheoriginalsurveynature,mainlythefactthatdatacamefrom anelectronicallyself-reportedquestionnairethatcouldbeaffected fromrecallbiaseffectandfromrespondentbiaswhenreporting subjectivesymptoms.Ontheotherside,theoverallItalian sam-pleincludedintheREVIVEsurveyrepresentsthelargestonenever included beforeabout VVAsymptomatology, being representa-tiveofthecurrentagestratificationoftheItalianpostmenopausal womenpopulation,aswellasoftheconditionanditsmanagement indifferentregionsinItalywithverydiversecultureintermsof sexualhealth[29].
Ourresultsdemonstratedthat,despitethecommonnessofVVA symptomsaftermenopauseanditssignificantimpactonqualityof lifeandsexualenjoyment,thisconditionremainsunderdiagnosed andundertreatedinItaly.Discussionofsymptomswithadoctorhas asignificantimpactontheincidenceofVVAdiagnosis,whilethe rateofdissatisfactionwithcurrentlyavailabletreatmentsremains relativelyimportant.Toeffectivelypromoteachangeofbehavior andofVVAperceptioninItalianwomen,bothpolicy-makersand cliniciansshouldconsiderthewaytosolvethedisputebetween expectationsandexperienceswithtreatments[33],togetherwith abalancededucationalprogramforpatientsaboutrealrisk-benefit profileofthecurrentlyavailableproducts.
Contributors
RENandMPdesignedthestudy.
REN,MP,NB,AC,CDC,SLandAMPdevelopedthemethodology. REN,NB,AC,CDC,SLandAMPsupervisedthecollectionofdata managedbyathirdparty.
MPperformedtheanalysis. RENwrotethemanuscript.
MP,NB,AC,CDC,SLandAMPcriticallyrevisedthemanuscript. Allauthorsgavefinalapprovaloftheversiontobepublished. Conflictofinterest
RossellaE.Nappihadafinancialrelationship(lecturer,member ofadvisoryboardsand/orconsultant)withBayerHealthCareAG, BoehringerIngelheim,ElyLilly,Endoceutics,GedeonRichter,HRA Pharma,MerckSharpe&Dohme,NovoNordisk,PfizerInc.,Procter &GambleCo.,ShionogiLimitedandTEVAWomen’sHealthInc.
MartireParticcoisanemployeeofShionogiItaly.
NicolettaBigliahadafinancialrelationship(lecturer,memberof advisoryboardsand/orconsultant)withGedeonRichter,Shionogi LimitedandItalfarmaco.
CostantinoDiCarlohadafinancialrelationship(lecturer, mem-berofadvisoryboardsand/orconsultant)withBayerHealthCare AG,GedeonRichter,HRAPharma,MerckSharpe&Dohme,Shionogi LimitedandTEVAWomen’sHealthInc.
AngeloCagnacci,StefanoLuisiandAnnaMariaPaolettideclare noconflictofinterest.
Funding
Financial support for the REVIVE Survey was provided by ShionogiLimited.
Ethicalapproval
Thecomprehensiveonlinequestionnairewasapprovedbythe correspondingaccreditedinstitutionalreviewboardsatthe respec-tiveinstitutions(UniversityofPavia,UniversityofTorinoSchool ofMedicine,UniversityofModena,UniversityofNaplesFederico II,UniversityofSienaandUniversityHospitalofCagliari).All sur-veyparticipantswereappropriatelyinformedofthenatureofthe studyandgaveinformedconsenttoparticipatebeforecompleting theonlinequestionnaire.
Provenanceandpeerreview
Thisarticlehasundergonepeerreview. Acknowledgements
The authors would like to thank Emili González-Pérez (TFS Develop),ScientificAdvisorandMedicalWriter,forhisassistance withmanuscriptpreparation.Sponsorshipandarticleprocessing chargesforthisstudywerefundedbyShionogi,Inc.
References
[1]D.J.Portman,M.L.S.Gass,VulvovaginalAtrophyTerminologyConsensus ConferencePanel,Genitourinarysyndromeofmenopause:newterminology forvulvovaginalatrophyfromtheInternationalSocietyfortheStudyof Women’sSexualHealthandtheNorthAmericanMenopauseSociety, Menopause21(2014)1063–1068,http://dx.doi.org/10.1097/GME. 0000000000000329.
[2]C.Castelo-Branco,N.Biglia,R.E.Nappi,A.Schwenkhagen,S.Palacios, Characteristicsofpost-menopausalwomenwithgenitourinarysyndromeof menopause:implicationsforvulvovaginalatrophydiagnosisandtreatment selection,Maturitas(2015),http://dx.doi.org/10.1016/j.maturitas.2015.05. 007.
[3]M.Lachowsky,R.E.Nappi,Theeffectsofoestrogenonurogenitalhealth, Maturitas63(2009)149–151,http://dx.doi.org/10.1016/j.maturitas.2009.03. 012.
[4]D.Bruce,J.Rymer,Symptomsofthemenopause,BestPract.Res.Clin.Obstet. Gynaecol.23(2009)25–32,http://dx.doi.org/10.1016/j.bpobgyn.2008.10.002. [5]M.B.MacBride,D.J.Rhodes,L.T.Shuster,Vulvovaginalatrophy,MayoClin.
Proc.85(2010)87–94,http://dx.doi.org/10.4065/mcp.2009.0413. [6]N.Santoro,J.Komi,Prevalenceandimpactofvaginalsymptomsamong
postmenopausalwomen,J.Sex.Med.6(2009)2133–2142,http://dx.doi.org/ 10.1111/j.1743-6109.2009.01335.x.
[7]R.E.Nappi,M.Lachowsky,Menopauseandsexuality:prevalenceofsymptoms andimpactonqualityoflife,Maturitas63(2009)138–141,http://dx.doi.org/ 10.1016/j.maturitas.2009.03.021.
[8]S.Palacios,Managingurogenitalatrophy,Maturitas63(2009)315–318,
http://dx.doi.org/10.1016/j.maturitas.2009.04.009.
[9]2011EUCensus,Eurostat,thestatisticalofficeoftheEuropeanUnion,2012.
http://ec.europa.eu/eurostat/web/population-and-housing-census/census-data/2011-census.
[10]R.E.Nappi,S.Palacios,Impactofvulvovaginalatrophyonsexualhealthand qualityoflifeatpostmenopause,Climacteric:J.Int.MenopauseSoc.17(2014) 3–9,http://dx.doi.org/10.3109/13697137.2013.871696.
[11]M.DiBonaventura,X.Luo,M.Moffatt,A.G.Bushmakin,M.Kumar,J.Bobula, Theassociationbetweenvulvovaginalatrophysymptomsandqualityoflife amongpostmenopausalwomenintheUnitedStatesandWesternEurope,J. WomensHealth(Larchmt)24(2015)713–722,http://dx.doi.org/10.1089/jwh. 2014.5177.
[12]S.J.Parish,R.E.Nappi,M.L.Krychman,S.Kellogg-Spadt,J.A.Simon,J.A. Goldstein,etal.,Impactofvulvovaginalhealthonpostmenopausalwomen:a reviewofsurveysonsymptomsofvulvovaginalatrophy,Int.J.Womens Health5(2013)437–447,http://dx.doi.org/10.2147/IJWH.S44579.
[13]S.A.Kingsberg,M.L.Krychman,Resistanceandbarrierstolocalestrogen therapyinwomenwithatrophicvaginitis,J.Sex.Med.10(2013)1567–1574,
http://dx.doi.org/10.1111/jsm.12120.
[14]R.E.Nappi,M.Kokot-Kierepa,Vaginalhealth:insights,views&attitudes (VIVA)—resultsfromaninternationalsurvey,Climacteric15(2012)36–44,
http://dx.doi.org/10.3109/13697137.2011.647840.
[15]NorthAmericanMenopauseSociety,Theroleoflocalvaginalestrogenfor treatmentofvaginalatrophyinpostmenopausalwomen:2007position statementofTheNorthAmericanMenopauseSociety,Menopause14(3Pt1) (2007)355–369,http://dx.doi.org/10.1097/gme.0b013e31805170eb(quiz 370-1).
[16]Wyeth,REVEAL:REvealingVaginalEffectsAtmid-Life,2009. [17]R.E.Nappi,E.A.Nijland,Women’sperceptionofsexualityaroundthe
menopause:outcomesofaEuropeantelephonesurvey,Eur.J.Obstet. Gynecol.Reprod.Biol.137(2008)10–16,http://dx.doi.org/10.1016/j.ejogrb. 2006.10.036.
[18]PfizerPharmaceuticals,Inc,HealthyWomenSurvey,2012,www. perosnalmenopauseanswers.com/healthy-women-survey.aspx(accessed 11.08.12).
[19]NovoNordisk,DataRevealtheNegativeEmotionalandPhysicalImpactthata SilentSymptomofMenopausehasonU.S.WomenandtheirPartners,2012. [20]R.E.Nappi,L.-Å.Mattsson,M.Lachowsky,R.Maamari,A.Giraldi,TheCLOSER
survey:impactofpostmenopausalvaginaldiscomfortonrelationships betweenwomenandtheirpartnersinNorthernandSouthernEurope, Maturitas75(2013)373–379,http://dx.doi.org/10.1016/j.maturitas.2013.05. 003.
[21]S.A.Kingsberg,S.Wysocki,L.Magnus,M.L.Krychman,Vulvarandvaginal atrophyinpostmenopausalwomen:findingsfromtheREVIVE(REalWomen’s VIewsofTreatmentOptionsforMenopausalVaginalChangEs)survey,J.Sex. Med.10(2013)1790–1799,http://dx.doi.org/10.1111/jsm.12190.
[22]R.E.Nappi,S.Palacios,N.Panay,M.Partico,TheREVIVE(REalWomen’sVIews ofTreatmentOptionsforMenopausalVaginalChangEs)SurveyinEurope: country-specificcomparisonsofpostmenopausalwomen’sperceptions, experiencesandneeds,Maturitas(inpreparation).
[23]K.S.Sutton,S.C.Boyer,C.Goldfinger,P.Ezer,C.F.Pukall,Tolubeornottolube: experiencesandperceptionsoflubricantuseinwomenwithandwithout dyspareunia,J.Sex.Med.9(2012)240–250, http://dx.doi.org/10.1111/j.1743-6109.2011.02543.x.
[24]R.E.Nappi,S.Palacios,N.Panay,M.Particco,M.L.Krychman,Vulvarand vaginalatrophyinfourEuropeancountries:evidencefromtheEuropean REVIVESurvey,Climacteric19(2016)188–197,http://dx.doi.org/10.3109/ 13697137.2015.1107039.
[25]A.Graziottin,Thechallengeofsexualmedicineforwomen:overcoming culturalandeducationallimitsandgenderbiases,J.Endocrinol.Investig.26 (2003)139–142.
[26]A.Caiazzo,M.Cardano,E.Cois,G.Costa,C.Marinacci,T.Spadea,etal., InequalitiesinhealthinItaly,Epidemiol.Prev.28(2004)1–161(i–ix).
[27]J.Simon,J.Komi,Vulvovaginalatrophy(VVA)negativelyimpactssexual function,psychosocialwell-being,andpartnerrelationships,in:Proc.North AmenricanMenopauseSoc.NAMS,Dallas,TX,USA,2007.
[28]F.Palma,A.Volpe,P.Villa,A.Cagnacci,WritingGroupoftheAGATAStudy, Vaginalatrophyofwomeninpostmenopause.Resultsfromamulticentric observationalstudy:theAGATAstudy,Maturitas83(2016)40–44,http://dx. doi.org/10.1016/j.maturitas.2015.09.001.
[29]R.E.Nappi,J.B.Verde,F.Polatti,A.R.Genazzani,C.Zara,Self-reportedsexual symptomsinwomenattendingmenopauseclinics,Gynecol.Obstet.Investig. 53(2002)181–187.
[30]C.DonatiSarti,A.Graziottin,M.Mincigrucci,E.Ricci,F.Chiaffarino,S.Bonaca, etal.,CorrelatesofsexualfunctioninginItalianmenopausalwomen, Climacteric:J.Int.MenopauseSoc.13(2010)447–456,http://dx.doi.org/10. 3109/13697130903491026.
[31]D.W.Sturdee,A.Pines,InternationalMenopauseSocietyWritingGroup,D.F. Archer,R.J.Baber,D.Barlow,etal.,UpdatedIMSrecommendationson postmenopausalhormonetherapyandpreventivestrategiesformidlife health,Climacteric14(2011)302–320,http://dx.doi.org/10.3109/13697137. 2011.570590.
[32]NorthAmericanMenopauseSociety,Estrogenandprogestogenusein postmenopausalwomen:2010positionstatementofTheNorthAmerican MenopauseSociety,Menopause17(March(2))(2010)242–255,http://dx.doi. org/10.1097/gme.0b013e3181d0f6b9.
[33]A.Coulter,C.Jenkinson,Europeanpatients’viewsontheresponsivenessof healthsystemsandhealthcareproviders,Eur.J.PublicHealth15(2005) 355–360,http://dx.doi.org/10.1093/eurpub/cki004.