September 2018 Photo Essay 1311
In vivo confocal microscopy of iris in
recessive cornea plana with anterior
synechiae
Enrico Bruni
1,2, Emilio Pedrotti
1, Paolo Plinio Di Sarro
1,
Mattia Passilongo
1, Giorgio Marchini
1Cite this article as: Bruni E, Pedrotti E, Di Sarro PP, Passilongo M, Marchini G. In vivo confocal microscopy of iris in recessive cornea plana with anterior synechiae. Indian J Ophthalmol 2018;66:1311-3.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected] circles (7 mm, 5 mm, and 3 mm, respectively) centered on
the maximum elevation of the posterior float, using the Mosaic delivery system (KXL II, Avedro Inc., Waltham, MA, USA). A mean keratometric reduction of 1.4 D [Fig. 1b and c] with a subsequent improvement in best‑corrected distance visual acuity from 6/12 to 6/7.5 was noted at 3‑months, with a subsequent stabilization up till 1‑year follow‑up [Fig. 1d]. No visually significant haze or endothelial cell loss was noted. The fellow eye was within normal limits.
Discussion
In our case, the treatment was centered on the maximum posterior float elevation. The use of varying treatment patterns including customized toric, asymmetric arcuates, and concentric circles has been described. In a majority of the earlier studies, the treatment was centered on the area of greatest curvature. However, centration of irradiation around the maximum point of posterior float elevation may be more intuitive since pachymetry as well as curvature is modulated by epithelial thickness and tear film.
Conclusion
In conclusion, we describe the clinical changes that ensue following PiXL over a 1‑year follow‑up. This ophthalmic image highlights the corneal tomographic changes and adds to the limited literature on this novel technique.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have
given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Roberts CJ, Dupps WJ Jr. Biomechanics of corneal ectasia and biomechanical treatments. J Cataract Refract Surg 2014;40:991‑8.
2. Sinha Roy A, Dupps WJ Jr. Patient‑specific computational modeling of keratoconus progression and differential responses to collagen cross‑linking. Invest Ophthalmol Vis Sci 2011;52:9174‑87. 3. Kanellopoulos AJ, Dupps WJ, Seven I, Asimellis G. Toric
topographically customized transepithelial, pulsed, very high‑fluence, higher energy and higher riboflavin concentration collagen cross‑linking in keratoconus. Case Rep Ophthalmol 2014;5:172‑80.
4. Nordström M, Schiller M, Fredriksson A, Behndig A. Refractive improvements and safety with topography‑guided corneal crosslinking for keratoconus: 1‑year results. Br J Ophthalmol 2017;101:920‑5.
5. Seiler TG, Fischinger I, Koller T, Zapp D, Frueh BE, Seiler T,
et al. Customized corneal cross‑linking: One‑year results. Am J
Ophthalmol 2016;166:14‑21.
Key words: Anterior synechiae, confocal microscopy, cornea plana, iris
We present a case of iris synechiae visualization with utilization of laser scanning vivo confocal microscopy (LSCM) in the recessive cornea plana. Autosomal recessive cornea plana (ARCP) is characterized by a flattened corneal surface associated with hyperopia and various anterior segment anomalities such as: corneal opacity, microcornea, anterior segment synechiae and a shallow anterior chamber.[1] The diagnosis is based on clinical and keratometric findings.[2]
Case
We examined confocal microscopy in a patient with cornea plana, anterior synechiae and shallow anterior chamber [Fig. 1]. Confocal microscopy was performed with HRT III Rostock Cornea Module (Heidelberg engineering, Germany). As previously reported by
1Eye Clinic, Department of Neurosciences, Biomedicine and Movement
Sciences, University of Verona, Ple Ludovico Antonio Scuro 10, 2Sacro
Cuore Don Calabria Hospital, Negrar, Verona, Italy
Correspondence to: Dr. Enrico Bruni, Sacro Cuore Don Calabria
Hospital, Via Don A. Sempreboni, 5, 37024 Negrar (Verona), Italy. E‑mail: [email protected]
Manuscript received: 26.03.18; Revision accepted: 19.05.18
Access this article online Quick Response Code: Website:
www.ijo.in DOI:
10.4103/ijo.IJO_346_18 PMID:
*****
1312 Indian Journal of Ophthalmology Volume 66 Issue 9 Vesaluoma, the Bowmann layer was absent[3] and keratocites
appeared fewer than in normal individuals. During the exam we discovered a fibrous‑like trabecular structure with: ramifications, interdigitations and scattered round processes below the corneal endothelium [Figs. 2‑5] that represent the iris tissue and the anterior iridocorneal synechiae
Discussion
Some researchers have tried to study the iris with a modified non‑contact laser scanning in vivo confocal microscopy (LSCM)[4] by changing the camera lens and increasing the working distance; however, the quality of images was subpair. Li et al. have reported iris ultrastructure in patients with anterior syneachiae[5] as revealed by LSCM. They found five patterns of iris ultrastructure: trunk‑like, branch/bush‑like, fruit‑like, epithelioid‑like, and deep, going from anterior to posterior. Our confocal microscopy images show four patterns of iris ultrastructure: in Figs. 2 and 3, a web‑like (trabecular) structure right below the corneal endothelium might represent the fibrous scar tissue of the anterior border layer of the iris synechiae [Figs. 2 and 3]. This pattern is similar to the tree‑branch structure found by Li et al., but our images show much thinner, much highly reflective branches, and wider empty spaces. Scattered round processes are visible and might represent pigment agglomerates. We were able to detect a deeper trunk [Fig. 4] and branch/bush‑like [Fig. 5] structures as reported by Li et al.
Figure 3: (a and b) Trabecular structures found below the corneal
endothelium with numerous pigment clumps (white arrows)
b a
Conclusion
In conclusion, we found a new trabecular structure right below the corneal endothelium [Figs. 2 and 3] that has never been seen in literature. This structure may represent the true synechiae between the anterior border layer iris and the corneal endothelium. While the images displayed by Li et al. show normal iris ultrastructure, our images display the stretched and fibrous iris tissue adherent to the corneal endothelium. We
Figure 1: Slit-lamp photograph of cornea plana with anterior synechiae.
Note the underlying iris tissues were dragged toward the corneal scars (adherent leukoma)
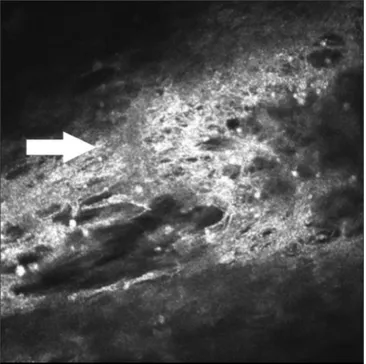
Figure 2: An example of fibrous web‑like (trabecular) structure with
thin branches (white arrows) in human iris with anterior synechiae by
in vivo LSCM
Figure 4: Trunk-like iris structure with scattered pigment clumps. Note
the support structure with thick arrangement (arrow) [Downloaded free from http://www.ijo.in on Monday, August 20, 2018, IP: 211.235.57.161]
September 2018 Photo Essay 1313
Department of Vitreo Retina, Aditya Birla Sankara Nethralaya, Kolkata, West Bengal, India
Correspondence to: Dr. Rupak Roy, Department of Vitreo Retina,
Aditya Birla Sankara Nethralaya, 147, Mukundapur, E. M. Bypass, Kolkata ‑ 700 099, West Bengal, India. E‑mail: [email protected]
Manuscript received: 13.01.18; Revision accepted: 26.04.18
Multimodal imaging in Multifocal
Best disease
Dhaivat Shah, Kumar Saurabh, Rupak Roy
Key words: Multicolor imaging, multifocal best disease, multimodal imaging
Multifocal Best disease (MBD) is a rare disease characterized by multiple sharply demarcated yellowish lesions in the posterior
Cite this article as: Shah D, Saurabh K, Roy R. Multimodal imaging in Multifocal Best disease. Indian J Ophthalmol 2018;66:1313-5.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected] Access this article online
Quick Response Code: Website: www.ijo.in DOI:
10.4103/ijo.IJO_70_18 PMID:
*****
were able to observe trunk‑like and branch/bush‑like structures at a deeper level into the iris as previously reported by Li et al. While deep structures are difficult to analyze due to limited penetration of laser light, LSCM is an excellent diagnostic tool
in autosomal recessive cornea plana and offers the possibility of visualizing iris ultrastructure when anterior synechiae are present.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ebenezer ND, Patel CB, Hariprasad SM, Chen LL, Patel RJ, Hardcastle RJ, et al., Clinical and molacular characterization of a family with autosomal recessive cornea plana. Arch Ophthalmol 2005;123:1248‑53.
2. Rantala E, Majander A. Anterior segment optical coherence tomography in autosomal recessive cornea plana. Acta Ophthalmol Scand 2015;93:232‑3.
3. Vesaluoma MH, Sankila EM, Gallar J, Muller RJ, Petroll WM, Mollanen JA, et al. Autosomal recessive cornea plana: In vivo corneal morphology and corneal sensitivity. Invest Ophthalmol Vis Sci 2000;41:2120‑6.
4. Sbeity Z, Palmiero PM, Tello C, Liebmann JM, Ritch R. Non‑contact
in vivo confocal scanning laser microscopy in exfoliation syndrome,
exfoliation syndrome suspect and normal eyes. Acta Ophthalmol Scand 2011; 89:241‑7.
5. Li M, Cheng H, Guo P, Zhang C, Tang S, Wang S. Iris ultrastructure in patients with synechiae as revealed by in vivo laser scanning confocal microscopy: In vivo iris ultrastructure in patients with Synechiae by Laser Scanning Confocal Microscopy. BMC Ophthalmol 2016;15(Suppl 1):46.
pole and beyond arcades. This is considered an atypical variant of Best vitelliform macular dystrophy (VMD).[1] This photo essay describes the multimodal imaging (MI) characteristic of MBD.
Case
A 14‑year‑old male presented with gradual loss of vision in both the eyes for 2 years. Best‑corrected visual acuity was 6/18, N6 both eyes. Color fundus photograph [Fig. 1a and b] showed multiple small round yellow subretinal lesions on the posterior pole extending beyond the arcades along with macular thickening. Multicolor image [Fig. 1c and d] showed greenish hue over the macula and multiple orange spots corresponding to yellow lesions. Blue‑light fundus autofluorescence (FAF) [Fig. 2a and b] showed multiple hyperautofluorescent lesions. Near‑infrared reflectance image [Fig. 3a and b] showed multiple white hyper‑reflective spots suggestive of alterations at retinal pigment epithelium (RPE) level, while green [Fig. 3c and d] and blue [Fig. 3e and f] reflectance image
Figure 5: Bush-like iris structure