Available online at
www.sciencedirect.com
journal homepage:
www.elsevier.com/locate/radcr
Case
Report
Primary
lymphoma
of
the
distal
radius
of
a
child:
imaging
features
Anna
Del
Poggio,
MD
a,
Luca
Facchetti,
MD
a,∗,
Alessandra
Ranza,
MD
b,
Fabio
Facchetti,
MD
PhD
c,
Ugo
Pazzaglia,
MD
a,
Maria
Pia
Bondioni,
MD
a,baDepartmentofMedicalandSurgicalSpecialties,RadiologicalSciencesandPublicHealth,PediatricRadiology, UniversityofBrescia,Brescia,Italy
bDepartmentofPediatricRadiology,ASSTSpedaliCivili,Brescia,Italy
cDepartmentofMolecularandTranslationalMedicine,SectionofPathology,UniversityofBrescia,SpedaliCivili, Brescia,Italy
a r t i c l e
i n f
o
Articlehistory: Received11July2018 Revised18August2018 Accepted26August2018 Keywords: Bone Lymphoma Paediatrica b s
t r a c t
Primarylymphomaofbone(PLB)isarareentity,definedasalymphomaconfinedtothe bonewithout evidenceofsystemicinvolvement.Thediseasecommonlyaffects middle-agedtoelderlypopulationanditaccountsforlessthan1%ofallmalignantlymphomas.We presentacaseofa10-year-oldchildaffectedbyPLBoftheforearmandthefrontalbone. CharacteristicimagingfeaturesofPLBandthemaindifferentialdiagnosiswerediscussed. © 2018TheAuthors.PublishedbyElsevierInc.onbehalfofUniversityofWashington.
ThisisanopenaccessarticleundertheCCBY-NC-NDlicense. (http://creativecommons.org/licenses/by-nc-nd/4.0/)
Introduction
Primarylymphomaofthebone(PLB)isararevariantof extra-nodalnon-Hodgkinlymphoma [1–3].AccordingtotheWorld HealthOrganizationclassification,lymphomainvolvingbone canbedividedintofourgroups:(1)singleskeletalsitewithout regionallymphnodeinvolvement;(2)multiple-bone
involve-Conflictofinterest:Theauthorsdeclarethattheyhavenoconflictofinterest. Funding:Thestudywasnotfunded.
Informedconsent:Informedconsentforpublicationofthiscasereportwasobtainedfromthepatient.
Ethicalapproval:Allproceduresperformedinthiscasereportwereinaccordancewiththeethicalstandardsoftheinstitutionaland/or nationalresearchcommitteeandwiththe1964Helsinkideclarationanditslateramendmentsorcomparableethicalstandards.
∗ Correspondingauthor.
E-mailaddresses: [email protected](A.D.Poggio),[email protected](L.Facchetti),[email protected]
(A.Ranza),[email protected](F.Facchetti),[email protected](U.Pazzaglia),[email protected](M.P.Bondioni).
mentwithoutvisceralorlymphnodeinvolvement;(3)bone lesionwithinvolvementofvisceralsitesor multiplelymph nodesatmultiplesites;and(4)patientwithknownlymphoma and bonebiopsy confirminginvolvementofbone.Groups1 and2areconsideredprimarylymphomasofthebone [3,4]. PLBaccountforlessthan1%ofallmalignantlymphomasand 7%ofmalignantbonetumors.Only4%-5%ofextranodal non-Hodgkin’slymphomasmanifestasPLB[2,5]andhistologically mostprimarybonelymphomasareprimarybonediffuselarge
https://doi.org/10.1016/j.radcr.2018.08.025
1930-0433/© 2018TheAuthors.PublishedbyElsevierInc.onbehalfofUniversityofWashington.Thisisanopenaccessarticleunderthe CCBY-NC-NDlicense.(http://creativecommons.org/licenses/by-nc-nd/4.0/)
B-celllymphomas(PBDLBCLs).Thediseasecommonlyaffects middle-aged to elderly population, with a median age of 48years [2].Inthisreport,wedescribethecaseofa 10-year-oldboyaffectedwithPLBpresentingwithararedouble in-volvementoftheforearmandthefrontalbone,focusingon PLBimagingfeaturesanddifferentialdiagnosis.
Case
report
A10-year-oldboycametoourattentionwitha2-month his-toryof pain inthe left forearm,in absence oftrauma. On physicalexamination,asubcutaneousswelling wasnotein thefrontalregion.Noothersymptomsorsignswerepresent; no history of fever,weight loss or sweating was reported. All bloodtests werenegative.Aradiography showed struc-turalalterationofthedistaldiaphysisoftheradius, consist-inginalternatedareasofhyperlucencyandsclerosis, associ-atedwithfocalinterruptionofthecortex(Fig.1aandb).The patientwasadmittedtothePediatricOrthopedicdepartment forfurtherinvestigations.Consideringtheradiography find-ings,CTwas performed.CTexaminationconfirmeda7-cm longstructuralalterationofthedistaldiaphysisoftheradium withamultilayeredperiostealreaction(lamelatedor“onion skin” periostealreaction),withbonerarefactionwithinthe le-sion,withoutinvolvementoftheepiphysis,jointandadjacent bones.ACTofthefrontalregionwasperformedshowinga secondosteolyticlesion,withlenticularmorphology, superfi-ciallyspreadingintosofttissuesanddeeplyintothe subdu-ralbone,withenhancementafteriodinatecontrastmedium administration(Fig.2a-d).A1.5TMRIwasperformedto evalu-atetheradiallesionthatappearedmarkedlyhypointenseon T1-weightedimagesandslighthyperintenseonT2-weighted images.There wasalsoperiosteal reactionwith softtissue edema. There was no soft-tissuemass (Fig. 3a-c).A Tech-netiumbonescanwasperformedforstagingofthedisease. Itshowedfocaluptakesintheradiallesionandinthefrontal bone(Fig.4).AdditionalinvestigationincludingwholebodyCT withcontrastmediumadministration,spinaltap,abone mar-rowaspirationandbiopsywereallnegative.Anopensurgical biopsyoftheradiallesionwasperformed,revealingatypical largecellsdiffuselyinfiltratingthebone. Immunophenotyp-ingshowedpositivityforCD20staining,weakexpressionof BCL2,andnegativityforCD3,CD10,CD30,BCL6,TdT (termi-naldeoxynucleotidyltransferase)andbroad-spectrum cytok-eratins;insituhybridizationforEpstein-Barrvirus wasalso negative.Tumorcellsshowedahighproliferationindex(90%) asdeterminedbyevaluationwithanti-Ki67antibody(Fig.5 a-d).Thepatientunderwentfourcycles ofpolychemotherapy accordingtothenon-Hodgkinlymphoma(NHL)97 protocol (consecutiveblocksofpolychemotherapycontaining dexam-ethasone,cyclophosphamide, methotrexate,vincristine, cy-tarabine,etoposide,ipofosfamide,ara-c,daunomycine,and in-trathecal therapy withmethotrexate, cytarabine,and pred-nisolone).Aftertwocyclesofchemotherapy,thechild under-wentre-stagingthatshowedpartialregressionofbothradial andfrontallesions.Afterthreemorecyclesofchemotherapy, asecondopensurgicalbiopsywasperformed;showing com-pleteremissionofthedisease,and MRIofthefrontalbone
Fig.1– Laterolateralprojection(a)andanteroposterior projection(b)radiographsoftheforearmshowinga structuralalterationofthedistaldiaphysisoftheradius withalternatedareasofhyperlucency(arrows)and sclerosis.Aregularperiostealreactionisevident (arrowheads).
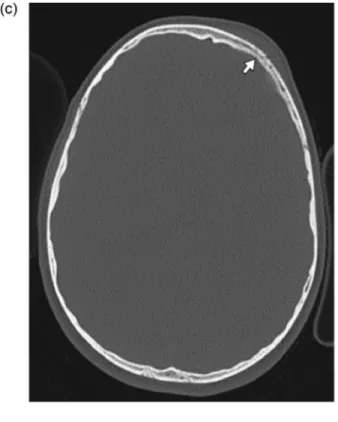
Fig.2– Axial(a)andcoronalreconstruction(b)CToftheforearm.A7-cmlongstructuralalterationofbonerarefactionofthe distaldiaphysisoftheradiumisevident.Multilayeredperiostealreaction(lamellatedor“onionskin” periostealreaction)is present(arrowheads).Thereisnoinvolvementoftheepiphysisjointandadjacentbones.Bonewindow(c)andsofttissue window(d)ofheadCTafteriodinatecontrastmediumadministration,showinganosteolyticarea(arrow)ofthefrontal boneassociatedwithalenticularshapedneoplasticlesion(arrowheads)spreadingintothesofttissue.
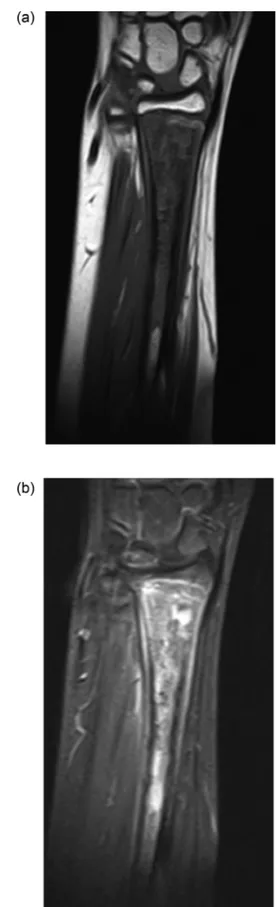
Fig.3– MRIoftheforearm,coronalT1(a)andT2 fat-saturated(b)weightedsequences.Theradiallesion
appearedheterogeneouslyhypointenseonT1-weighted
imagesandmainlyhyperintenseonT2-weightedimages.
Thereisnosoft-tissuemass.
Fig.4– Technetiumbonescan.Therearefocaluptakesboth intheradialandinthefrontalbonelesions(arrows).No otherpathologicuptakewasrecognized.
andoftheforearmconfirmedtheabsenceofrecurrence.At 46monthsoffollow-up,thepatientwashealthywithout evi-denceofthedisease.
Discussion
Primary lymphoma of boneis a rare primary bone malig-nancyandisdefinedasalymphomathatisconfinedtothe boneor bonemarrow without evidenceof concurrent sys-temicinvolvement.PLBhasamorefavorableprognosisthan systemiclymphomawithboneinvolvement,with5-year sur-vivalgreaterthan95% [6].Inourcase,norecurrencewas de-tectedafter3yearsoffollow-up.
PLBsitesofboneinvolvementarefemur(27%),pelvis(15%), tibia/fibula(13%),humerus(12%),spine(9%),mandible(2%), radius/ulna(1%),scapula (1%),andskull (1%) [2,3].The ra-diusinvolvementisexceptionallyrare,andDahlin[7]reported only6casesoutofaseriesof905malignantlymphomaof thebone.Themetaphysisisthemostcommonsiteof occur-renceinlongbones.Themostcommonlyaffectedsitesarethe sameforPLB,Ewingsarcoma,osteosarcoma,andtheradiusis araresiteofinvolvementinallofthem[8,9].
TheappearanceofPLBatimagingisusuallyvariableand nonspecific [10, 11] and metastatic lymphoma is indistin-guishablefromprimarybonelymphomawithoutwhole-body stagingtodetectotherdiseaselocalizations.Radiological find-ingsincludewidespreadlyticinfiltrationinthecorticalbone (lytic-destructivepattern70%)orscleroticboneresponse ac-companyinglytic permeation (mixed lytic-sclerotic pattern 28%)asinourcase [10].ThemajorityofPLBpresentaslytic lesion,moreoftenlocalizedinlongbonemetaphysis,withan infiltrativeormoth-eatenpatternofdestructionand aggres-siveperiostealreaction [10,12].Thelesioncanbeassociated
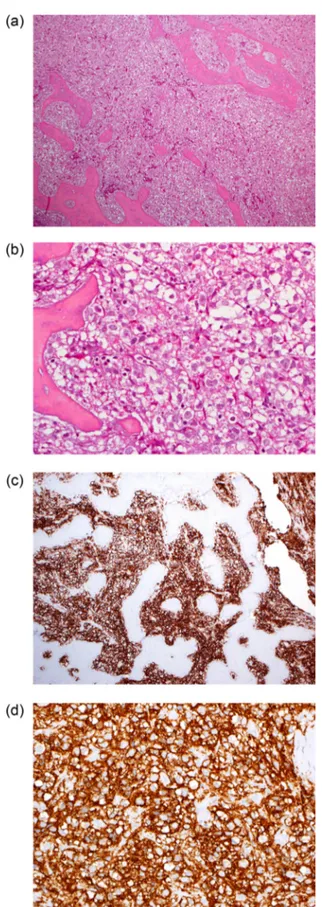
Fig.5– Low(a,c)andhigh(b,d)powerviewofbonebiopsy stainedwithhematoxylin-eosin(a-b)andanti-CD20(c-d). ThemedullaryspacesarefilledbylargeatypicalBcells, stronglypositiveperCD20.
toasofttissuemass [11]asforroundcelltumors(including Ewingsarcoma),amongwhichlymphomaisanexample.On MRI the lesion mostoften haslow signal intensity on T1-weightedimagesanditappearsslightlyhyperintenseon T2-weighted images [11,13].Thebone-marrow involvementis bestdemonstratedonT1-weightedimagesrevealingareasof lowsignalintensitywithinthemarrow,whileonT2-weighted images these areas appear bright. After administration of Gadolinium,T1fat-saturatedsequencescandemonstrate ar-eas ofenhancementwithinthe lesion [10]. Inourcasethe lesionsdidnotshow apermeativepattern whichistypical ofboneinfiltrativeneoplasms,but ratheranirregular corti-caldisruptionwithperiostealreactionandonion-skinpattern. Therewassofttissueedemaandnosofttissuemass.The le-sionswereveryhypointenseinT1-weightedimagesandslight hyperintenseinT2-weightedimages.
Inthefirstdecadeoflife,Ewingsarcomaandosteosarcoma arethemostcommonprimarybonetumors,but malignant lymphomaoftheboneisthethirdmostcommon [7]andit shouldbealwaystakeninconsideration.Metastatic neurob-lastoma,eosinophilicgranulomaandosteomyelitismustbe consideredinthedifferential diagnosistoo.Inourcasethe imagingfindingsand thesymptomsdidnotsuggestthe di-agnosisofEwingsarcomabecauseofthelackofan infiltra-tivepattern,feverand increasederythrocyte sedimentation rate [14].Thehigh-gradeintramedullaryosteosarcomacould mimicPLB. Osteosarcoma commonlypresents with diffuse bonedestructionalternatedtoareasofsclerosisand fociof hemorrhagesandnecrosiscanbeseen.Osteomyelitisinthe earlystagestypicallydemonstrateanosteolyticlesionlocated adjacenttothegrowthplateinthemetaphysisbutwithtime progressivesclerosiscanbeseenaroundthelyticlesion[15].
Insummary,primarylymphomaofboneisararecondition, particularlyinthepediatricpopulation.Theradiographic ap-pearanceofPLBisvariablebutthelytic-destructivepatternis moretypical.AlthoughosteosarcomaandEwingsarcomaare morecommon,asolitarylyticlesioninalongboneshould al-waysraisethesuspicionofPLB.
Supplementary
materials
Supplementary materialassociatedwiththis articlecanbe found,intheonlineversion,atdoi:10.1016/j.radcr.2018.08.025.
R E F E R E N C E S
[1] DöllC, WulffB, RösslerJ, SchaperJ, HaversW.PrimaryB-cell lymphomaofboneinchildren.EurJPediatr
2001;160(4):239–42.
[2] BhagavathiS,FuK.Primarybonelymphoma.ArchPatholLab Med2009;133(11):1868–71.
doi:10.1043/1543-2165-133.11.1868.
[3] DemircayE,HornicekFJ,MankinHJ,DegrootH.Malignant lymphomaofbone:areviewof119patients.ClinOrthop RelatRes2013;471(8):2684–90.
[4] deCamargoOP, dosSantosMachadoTM, CrociAT.Primary bonelymphomain24patientstreatedbetween1955and 1999.ClinOrthopRelatRes2002;397:271–80.
[5] DesaiS, JambhekarNA, SomanCS, AdvaniSH.Primary lymphomaofbone:aclinicopathologicstudyof25cases reportedover10years.JSurgOncol1991;46(4):265–9.
[6] LonesMA,PerkinsSL,SpostoR.Non-Hodgkin’slymphoma arisinginboneinchildrenandadolescentsisassociated withanexcellentoutcome:aChildren’sCancerGroupreport. JClinOncol2002;20(9):2293–301.doi:10.1200/JCO.2002.06.017.
[7] DahlinDC, UnniKK, InwardsCY.Bonetumors:general aspectsanddataon10,165cases.Philadelphia:Wollters Kluwer/LippincottWilliams&Wilkins;2010.
[8] MurpheyMD,RobbinMR,McRaeGA,FlemmingDJ, TempleHT,KransdorfMJ.Themanyfacesofosteosarcoma. Radiographics1997;17(5):1205–31.
doi:10.1148/radiographics.17.5.9308111.
[9] MurpheyMD,SenchakLT,MambalamPK,LogieCI, Klassen-FischerMK,KransdorfMJ.Fromtheradiologic pathologyarchives:ewingsarcomafamilyoftumors: radiologic-pathologiccorrelation.Radiographics 2013;33(3):803–31.doi:10.1148/rg.333135005.
[10]KrishnanA,ShirkhodaA,TehranzadehJ,ArminAR,IrwinR, LesK.Primarybonelymphoma:radiographic-MRimaging correlation.Radiographics2003;23(6):1371–83discussion 1384-1387.doi:10.1148/rg.236025056.
[11]MulliganME,McRaeGA,MurpheyMD.Imagingfeaturesof primarylymphomaofbone.AJRAmJRoentgenol 1999;173(6):1691–7.doi:10.2214/ajr.173.6.10584821.
[12]PhillipsWC,KattapuramSV,DoseretzDE.Primary
lymphomaofbone:relationshipofradiographicappearance andprognosis.Radiology1982;144(2):285–90.
doi:10.1148/radiology.144.2.7045976.
[13] Cıraklı A, Elli M, Dabak N, Canbaz Tosun F, Da˘gdemir A, Cıraklı S.Evaluation of primary bone lymphoma and the importanceofpositronemissiontomography.ActaOrthop TraumatolTurc2014;48(3):371–8.
[14] MaheshwariAV, ChengEY.Ewingsarcomafamilyoftumors. JAmAcadOrthopSurg2010;18(2):94–107.
[15]KhannaG,SatoTSP,FergusonP.Imagingofchronicrecurrent multifocalosteomyelitis.Radiographics2009;29(4):1159–77. doi:10.1148/rg.294085244.