CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports20(2016)80–83
ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
jo u r n al ho me p a g e :w w w . c a s e r e p o r t s . c o m
Hepatoblastoma
of
the
adult
with
pericardial
metastasis:
A
case
report
Andrea
Celotti
∗,
Gian
Luca
Baiocchi,
Marco
Ceresoli,
Michele
Bartoli,
Silvia
Ulinici,
Nazario
Portolani
DepartmentofMedicalandSurgicalSciences,SurgicalClinic,UniversityofBrescia,25123Brescia,Italy
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10December2015 Accepted13January2016 Availableonline19January2016
Keywords: Hepatoblastoma
Hepatoblastomaoftheadult Livertumor
Diaphragmrepair Biologicmesh
a
b
s
t
r
a
c
t
BACKGROUND:Hepatoblastomaisthemostfrequentlivertumorinchildren,butveryrareintheadult andassociatedwithanunfavorableprognosis.Thediagnosisisalwayspostoperativeorpostmortemand biopsyisnotuseful.Surgeryistheonlyacceptedtreatment.
CASEPRESENTATION:Ourpatientunderwentsurgeryinthesuspectoflivermetastasisfromaprevious gastriccancer.Surgeryconsistedinleftlobectomywithpartialdiaphragmresectionandpartial peri-cardiectomyforapericardiallesion,foundaftertheopeningofthethorax.Thediaphragmdefectwas correctedwithabiologicalmesh.
RESULTS:Thehistopathologicalexaminationindicatedhepatoblastomaoftheadultwithpericardial metastases.Thepatientwasasymptomaticandwithoutrecurrenceafter21monthsoffollowup. CONCLUSION:Thehepatoblastomaoftheadultisrelatedtoapoorprognosiswithmediansurvivaltime lessthan5months.Surgeryistheonlycurativetreatment,butinmanycasestumorresectionrequires complexoperations.Vascularandthoracicexpertisecouldbeusefulinthemanagementof hepatoblas-toma.
©2016TheAuthors.PublishedbyElsevierLtd.onbehalfofIJSPublishingGroupLtd.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Hepatoblastoma(HB)isararetumor,butthemostfrequentliver tumorinchildhood.
Itsusuallyoccursininfantsunder3yearsofageandthe5years overallsurvivalrateinchildrenwithnondisseminatedtumorsis closeto70%[1].
Hepatoblastomainadultisveryrare,withanunfavorable prog-nosis[2].Inliteratureaboutsixtycaseshavebeendescribed. In 1958Barnettetal.[3]reportedthefirstcaseinayoungman,who diedafteronemonthfromthediagnosisduetoacompleteliver replacebythetumorspreading.TheprognosisofHBintheadultis extremelypoor,becausemostcasesareunresectableatthe diag-nosisandnon-surgicaltreatmentshaveonlyapalliativerole[4].
Thisreportdescribesacaseofa68year-oldmanwho under-wenttotalgastrectomyforgastriccancer.Subsequently,thepatient underwent leftliver lobectomy after1 year forsuspected liver metastases, but the definitivehistological examination showed hepatoblastoma.
Abbreviations: HB,hepatoblastoma;MRI,magneticresonanceimaging;HCV, hepatitsCvirus;HBV,hepatitisBvirus;GOT,glutamicoxaloacetictransaminase; GPT,glutamicpyruvictransaminase;AFP,alpha-fetoprotein;PO,postoperative.
∗ Correspondingauthorat:DepartmentofMedicalandSurgicalSciences,Surgical Clinic,UniversityofBrescia,IIIChirurgia,SpedaliCivilidiBrescia,P.leSpedaliCivili 1,25123Brescia,Italy.Fax:+39030396011.
E-mailaddress:[email protected](A.Celotti).
2. Casereport
This is the case of a 68 year-old man who underwent, in January2012atanotherInstitution,totalgastrectomywith Roux-en-YesophagojejunostomywithD2lymphadenectomyforgastric cancer.Histologicalexaminationshowedgastricadenocarcinoma, intestinaltype,withlowdifferentiation(G3),withmetastasisto theregionalnodes(pT3N3M0).
Patient received adjuvant chemotherapy with 10 cycles of FOLFOX.InDecember 2012,during theoncologicalfollow-up, a suspected2cmlivermetastaseswasdiscovered.Forthisreason, the patient started 8 cycles of FOLFIRI. In October 2013, new MRIrevealed anincreased livermetastases upto 5cm (Fig.1). Noothercancerlocalizationswerefound.Patientwasreferredto ourhospital.Bloodexaminationsrevealednegativeserologyfor HCVandHBV,normallevelsofGOT,GPT,bilirubin,albumin.AFP levelwas1231UI/mL.Hehad nohistory ofalcohol intake.MRI wasre-evaluatedbyhepato-biliarydedicated-radiologistsandthe malignant natureofthelesion, withthefeatures of metastases wasconfirmed.InNovember2013thepatientunderwentsurgery. Peritonealexplorationrevealedalargesolidlesionofthesecond liversegment,completelyexophytic,withdiaphragminfiltration (Fig.2).Intraoperativeliverultrasoundwasnegativeforoccultliver metastasesandnoperitonealcarcinomatosisorothercancer local-izationswerefound.Theoperationconsistedofleftlobectomyand diaphragmresection.
http://dx.doi.org/10.1016/j.ijscr.2016.01.010
2210-2612/©2016TheAuthors.PublishedbyElsevierLtd.onbehalfofIJSPublishingGroupLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
CASE
REPORT
–
OPEN
ACCESS
A.Celottietal./InternationalJournalofSurgeryCaseReports20(2016)80–83 81
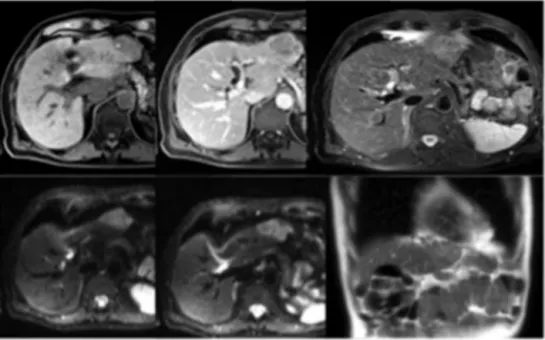
Fig.1.RMNimaging:typicalradiologicalaspectofalivermetastasis.NootherlocalizationsareevidentintheRMN.
Fig.2. ExophiticlesionoftheIIsegmentwithdiaphragminfiltration.
Thefirststepwastheincisionofthediaphragmsurroundingthe liverlesion,untilacompletedetachmentofthetumoren-blocwith apieceofdiaphragm.Duringthesurgery,throughthe diaphrag-maticdefect,apericardialnoduleofabout4cm wasdiscovered alongtheinfero-lateralcardiacmargin(Fig.3).
Althoughthepresenceofasecondneoplasticlocalization,aR0 surgerywasconsideredfeasible.Inferiorcavaveinwasisolated until rightathrium and anextended pericardiectomy was per-formed,fromtheupperrightathriumtotheinferiorcardiacmargin. Topreventcardiactamponade,theparietalpleurawassuturedto thepericardialmargin.Finallyleftliverlobectomywascompleted. Thedefectofthediaphragmwasrepairedusinga 10×10cmof bovinepericardium(Fig.4),suturedwithEthyleneTerephthalate. Abdominalandthoracicdrainswereplaced.Postoperativecourse wasuneventfulanddrainswereremovedon7thpostoperativeday (PO).Thepatientwasdischargedon13thPO,withoutproblems. AFPlevelwasremarkablydecreasedat290UI/mLatthedischarge. Themacroscopicpathologyreportshoweda6×4cmlivermass anda3.5×3cmpericardialnodewiththesamehistological fea-tures. Bothlesions werecomposed by double cell-populations: columnarandvacuolated cellsandpleomorphic cells.Extensive
Fig.3. Pericardialnodule.TheHarringtonretractorholdsthehearttopermitthe exposureoftheinferiorcavavein.
CASE
REPORT
–
OPEN
ACCESS
82 A.Celottietal./InternationalJournalofSurgeryCaseReports20(2016)80–83
Fig.5.(A,B)Hematoxylineosinofthelivertumor;(C,D)anti-hepatociticantigenandalphaphetoproteinpositivityrespectivelyofthelivertumor;(E,F)hematoxylineosin pericardialmetastasis.
necrosisandcalcificareaswerefound.Immunohistochemistrywas positivefor:anti-hepatociticantigen,alphaphetoprotein,vimentin, CD10andcytokeratin8e19andnegativeforcytokeratin7, cytoker-atin20,CDX-2,PLAP,betaHCG,OCT4,TCL1,CD30,calretinin.Final diagnosiswasadulthepatoblastomawithpericardialmetastasis (Fig.5).Wediscussedthecasewiththeoncologistsandno adju-vanttherapywasstarted.After21monthspatientisdisease-free andasymptomatic.
3. Discussion
Hepatoblastomaisthemostcommonlivertumorinchildren, andoccursespeciallyinpatientsunder5yearsofage[1].
Nowadaysinchildren,theadvancesinchemotherapy,especially toallowcompletesurgicalresectioneveninadvancedtumors,have increasedtheoverallsurvivalfrom30%toover80%[5].Inadult, HBisveryrareandinliteratureonly62casesaredescribedand presentsanextremelypoorprognosis.
PatientswithHBusuallyhaverightupperquadrantpain,often inpresenceofabdominalmass.Insomecasesacutepresentation withhemoperitoneumisreported[6–8].
Imagingisnotusefulfor thediagnosis,becauseHBpresents similarcharacteristicstootherscommonlivertumorssuchas hep-atocarcinomaormetastases[8].
InthiscaseMRIwastypicalforamalignantlesionwiththe fea-turesof asecondary livertumor,especially thepresenceofthe T1-hyperintensityperipheralringwasstronglysuspectedfor sec-ondarism.BloodexaminationofthepatientrevealedanAFPlevel of1231UI/mL,withoutliverdiseaseandhepresentedahistoryof gastriccancer.Thisdatacouldberelatedtothepreviousoncologic history,becauseinliteraturearereportedcasesofgastriccancer alpha-fetoproducing[9–11].AnywayYamazakietal.[12]declared thatAFPlevelswereoftenelevatedinHB,soitcouldbeusedasa serologicalmarkerlikeforthehepatocarcinoma.
Consideringitsrarity,thelackofparticularradiologicalfeatures andtheuncertainroleofAFP,thepreoperativediagnosisofHBin theadultisquiteimpossiblewithoutsurgeryorbiopsy.
Anywaytheuseofthebiopsyisdebatableinliterature,because inthepresenceofapotentiallyresectablelivermalignancy,surgery shouldbeperformedandthepostoperativediagnosisconsidered adequate.Mondragonetal.[13]reportedacaseofapatientdied afterpercutaneousbiopsyformultifocalHB.
The core treatment of this tumor is surgery as in pedi-atricpatients. Inchildrensurgeryisusuallyperformedafterpre
CASE
REPORT
–
OPEN
ACCESS
A.Celottietal./InternationalJournalofSurgeryCaseReports20(2016)80–83 83
operativechemotherapy, butin theadultthere is no standard-izedmanagement ofHB.In many cases,in ordertoachieve an R0resection,majorhepatectomiesoren-blocresectionsof adja-centorganssuchasdiaphragm,stomach,esophagus,pericardium, orspleenareneeded.Andersonetal.[14]reportedacaseofan extensiveresectionoftheleftliverlobe,withdemolitionofleft diaphragm, partialpericardiectomy, distal esophagectomy, par-tialgastrectomy,splenectomyand omentectomy.Regardingthe chemotherapytreatment,thereisnoagreementinliteratureonits use.InthereviewofYamazakietal.[12].noresponseto chemother-apywasobservedinanycase andtheauthorconcludedthatan excisionofthetumorshouldbeconsidered,withoutpreoperative chemotherapyandtumorpuncture.
InsteadNakamura etal.[4]reportedacaseofapatientwith a4yearssurvivalaftermultimodaltreatmentwithneoadjuvant chemotherapy,liverresectionandpostoperativechemotherapy.
HBpresentsapoorprognosisintheadultduetoitsmetastatic behaviororthelocalaggressiveness.InthereviewofWangetal. themediansurvivaltimefor27patientswithavailablefollowup was4months,with1-yearsurvivalof29.6%[2].Rougemontetal. [6]reported34patientswithamediansurvivaltimeof2months andwitha1-yearsurvivalof24%.Likeinourcase,inliteratureare reportedjusttwocasesofdiaphragmresectionduetothe inva-sionofthetumor,butnoinformationsaboutreconstructionare discussed[14,15].
Inthiscasethediaphragmdefectwastoobiggertoallowadirect closure,soabiologicalmeshofbovinepericardiumwasused.This methodisgenerallyadopted,inourDivision,inthecasesoflarge hepatocarcinomasoftheposteriorsegmentswithgoodresults.
Inliteraturetheuseofbovinepericardialmeshseemtohave goodoutcomeintermsofbiocompatibility,high-tensilestrength and easy use, so it could be recommended in many cases of diaphragmreconstruction[16–18].
Inthecaseofourpatienttheuseofthismaterialwas particu-larlyappropriatebecauseafterpericardiectomy,theheartwould be directly into contact of a soft biological mesh, but with a high-tensilestrength.Inthiscase,thepericardialmetastasectomy allowedacurativesurgery.Thepatient,after21monthsoffollow up,wasasymptomaticandwithoutrecurrence.Thisisthecaseof metastatichepatoblastomawiththelongerdisease-freesurvivalin theliterature.
4. Conclusion
Theprognosisofthehepatoblastomaintheadultis unfavor-ablewithmediansurvivaltimelessthan5months.ManyHBare unresectablesatdiagnosis,becauseoflocalaggressivebehavioror metastaticspread.Surgeryrepresentsthegoldstandardtreatment, butinmanycasestumorresectionrequirescomplexoperations. Vascularandthoracicexpertisecouldbeusefulinthemanagement ofhepatoblastoma.
Conflictofinterest
Theauthorsdeclarenopotentialconflictsofinterestrelevantto thisarticle.
Funding
Nofundingareemployed.
Ethicalapproval
Thisisnotaresearchstudy. Consent
Weobtainedawrittenandsignedconsenttopublishthiscase report.
Authorcontribution
AlltheAuthorsmadesubstantialcontributionstoconception anddesignofthestudy,CelottiA.andCeresoliM.conceivedthe studyand wrotethepaper; BartoliM.andUlinici S. performed Literaturesearch;BaiocchiG.L.andPortolaniN.reviewedthepaper. Guarantor
AndreaCelotti. References
[1]Y.Zhang,W.L.Zhang,D.S.Huang,L.Hong,Y.Z.Wang,X.Zhu,etal.,Clinical
efficacyandprognosisfactorsforadvancedhepatoblastomainchildren:a
6-yearretrospectivestudy,AsianPac.J.CancerPrev.14(8)(2013)4583–4589.
[2]Y.X.Wang,H.Liu,Adulthepatoblastoma:systemicreviewoftheEnglish
literature,Dig.Surg.29(4)(2012)323–330.
[3]W.H.Barnett,E.E.Erickson,B.Halpert,Embryonictumoroftheliverinan
adult,Cancer11(March–April(2))(1958)306–309.
[4]S.Nakamura,M.Sho,H.Kanehiro,T.Tanaka,K.Kichikawa,Y.Nakajima,etal.,
Adulthepatoblastomasuccessfullytreatedwithmultimodaltreatment,
LangenbecksArch.Surg.395(November(8))(2010)1165–1168.
[5]P.Czauderna,D.Lopez-Terrada,E.Hiyama,B.Häberle,M.H.Malogolowkin,
R.L.Meyers,etal.,Hepatoblastomastateoftheart:pathology,genetics,risk
stratification,andchemotherapy,Curr.Opin.Pediatr.26(February(1))(2014)
19–28.
[6]A.L.Rougemont,V.A.McLin,C.Toso,B.E.Wildhaber,etal.,Adult
hepatoblastoma:learningfromchildren,J.Hepatol.56(June(6))(2012)
1392–1403.
[7]M.H.Zheng,L.Zhang,D.N.Gu,H.Q.Shi,Q.Q.Zeng,Y.P.Chen,etal.,
Hepatoblastomainadult:reviewoftheliterature,J.Clin.Med.Res.1(April
(1))(2009)13–16.
[8]B.O.Al-Jiffry,Adulthepatoblastoma:acasereportandliteraturereview,Int.J.
Surg.CaseRep.4(2)(2013)204–207.
[9]X.Liu,M.Yang,J.Gao,S.Zhang,Y.Xi,etal.,Clinicopathologicfeaturesand
prognosisof51patientswith␣-fetoprotein-producinggastriccancer,
ZhonghuaZhongLiuZaZhi.37(March(3))(2015)231–234.
[10]W.Sun,Y.Liu,D.Shou,Q.Sun,J.Shi,L.Chen,etal.,AFP(alphafetoprotein):
whoareyouingastrology?CancerLett.357(February(10))(2015)43–46.
[11]K.Kono,H.Amemiya,T.Sekikawa,H.Iizuka,A.Takahashi,H.Fujii,etal.,
Clinicopathologicfeaturesofgastriccancersproducingalpha-fetoprotein,Dig.
Surg.19(5)(2002)359–365,discussion365.
[12]M.Yamazaki,M.Ryu,S.Okazumi,F.Kondo,A.Cho,T.Okada,etal.,
Hepatoblastomainanadultacasereportandclinicalreviewofliteratures,
Hepatol.Res.30(November(3))(2004)182–188.
[13]R.MondragónSánchez,R.BernalMaldonado,L.A.SadaNavarro,A.I.
Hernández,H.HurtadoAndrade,T.CortésEspinoza,etal.,Epithelial
hepatoblastomasinadult,Rev.Gastroenterol.Mex.59(1994)231–235.
[14]B.B.Anderson,F.Ukah,A.Tette,S.G.Villaflor,D.Koh,P.Seton,etal.,Primary
tumorsoftheliver,J.Natl.Med.Assoc.84(February(2))(1992)129–135.
[15]K.S.Reddy,P.K.Karak,S.Sharma,R.C.Rao,M.Vijayaraghavan,P.Sahni,etal.,
Epithelialhepatoblastomainamiddleagedwoman,Trop.Gastroenterol.18
(October–December(4))(1997)163–164.
[16]P.Santillán-Doherty,R.Jasso-Victoria,A.Sotres-Vega,R.Olmos,J.L.Arreola,D.
Garc-ia,etal.,Repiarofthoracoabdominalwalldefectsindogsusingabovine
pericardiumbioprosthesis,Rev.Invest.Clin.47(November–December(6))
(1995)439–446.
[17]B.Wiegmann,P.Zardo,N.Dickgreber,F.Länger,C.Fegbeutel,A.Haverich,
etal.,Biologicalmaterialsinchestwallreconstruction:initialexperiencewith
thePeri-GuardRepairPatch,Eur.J.Cardiothorac.Surg.37(March(3))(2010)
602–605.
[18]K.B.Ricci,R.Higgins,V.C.Daniels,A.Kilic,etal.,Bovinepericardial
reconstructionofthediaphragmafterahearttransplant,Exp.Clin.
Transplant.12(June(3))(2014)277–278.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.