and Perception Technologies
PERCeptual RObotics Laboratory
Socially-Oriented Technology Framework
for Rehabilitation of Children
during Developmental Ages
Ilaria Bortone
Submitted in part fulfilment of the requirements for the degree of Doctor of Philosophy in Emerging Digital Technologies,
The past decade has seen the emergence of rehabilitation treatments using virtual reality en-vironments. One of the advantages in using this technology is the potential to create positive motivation, by means of engaging environments and tasks shaped in the form of serious games. However translation into clinical practice is poor and uptake is dependent on a complex rela-tionship between all stakeholders [1]. Strength of evidence for clinical effectiveness and us-ability has been cited as an important factor influencing translation of rehabilitation research into clinical practice [2]. In this work, we propose an innovative technological framework that would embrace all the aspect concerning the rehabilitation process: from education to diag-nosis to therapy. Under the proposed ”Socially-Oriented Technology” framework, we pursued the following objectives: to assess the potential abilities of a co-creative approach in promot-ing healthy body consciousness in both typically developpromot-ing and autistic children in order to prevent injuries; to investigate the role of cutting-edge technologies, like virtual reality and haptic interfaces, to improve rehabilitation process in children with developmental disorders. An innovative model for school-based postural education project (PoSE) to promote healthy behaviors among middle school students and their families and to moderate postural diseases was investigated, consisting in interactive lessons on back posture and good principles both in class and at home. A participatory approach was used to evaluate attempts to involve all who have a stake in outcomes in order to take action and effect change. The strength of the par-ticipatory approach used in this study lies in the contribution to empowerment social change. Preliminary experimental sessions have been conducted with children with autistic disorders in order to arise their body consciousness. Finally, a novel Neuro Motor Rehabilitation System for children with neuro motor impairments (both Cerebral Palsy, CP, and Developmental Dys-praxia, DD), that is based on serious games in immersive virtual reality with haptic feedback, has been introduced. The system design is intended to enhance involvement and engagement of patients, to provide congruent multi-sensory afferent feedback during motor exercises, and to benefit from the flexibility of virtual reality in adapting exercises to the patient’s needs. The system takes advantage of immersive virtual reality systems and robotic haptic devices to en-hance involvement and engagement of patients, to provide a congruent multi-sensory afferent feedback during motor exercises, and to benefit from the flexibility of virtual scenarios for adapting the motor exercises to the needs of the patient. An experimental rehabilitation session conducted with CP/DD children has been performed to evaluate usability of the system and
derstand results in terms of gaming usability and performance of the proposed motor task, we compared CP/DD performance with both TD and the AD control group. The obtained results show the system was compliant with different levels of motor skills and allowed patients to complete the experimental rehabilitation session. In addition, the proposed exercises and the difficulty of the serious games showed to be sensitive to the different levels of motor functions: overall, CP group obtained lower performance than the TD and AD group, according to the dif-ferently developed motor abilities of the three groups. Furthermore, the use of a VR system in the presented system allowed for an immediate measurement and recording of patient’s upper limb movements. These kinematic measurements were used to design a set of metrics and mo-tor tasks, based on the exercises proposed in the serious games, to be introduced as an outcome of the patients’ motor functions. The developed kinematic assessment was then experimentally applied on two groups of eight TD children and eight CP/DD children. Results showed that the adopted metrics were in line with the difference in motor functions expected between the TD group and the CP/DD group. A Randomized Controlled Single-Blind Crossover Clinical Trial has been proposed to investigate the usability and effectiveness of serious games and wearable haptic interfaces for neuro motor rehabilitation of children with neuro motor disorders.
I would like to express my sincere gratitude to all of you who have contributed with your time and experience and in many other ways supported me in my work with this thesis. I particularly would like to thank:
• My supervisor for his patience and his confidence in my work
• My family for their unconditional love
• My colleagues - almost friends - who share with me part of this long journey
• All children and parents who participated in the intervention study and contributed with your time and efforts to this research project. Without you this thesis would not have been possible.
To My Family & to the only little creature who changed my life, Angelica
It is not far, it is within reach, Perhaps you have been on it since you were born and did not know, Perhaps it is everywhere on water and on land. Walt Whitman (Song of Myself, Part 46)
Abstract i
Acknowledgements iii
1 Introduction 1
1.1 Motivation and Objectives . . . 1
1.2 Contributions . . . 6
1.3 Statement of Originality . . . 8
1.4 Publications . . . 8
2 Background and Literature 11 2.1 Social Innovation . . . 11
2.1.1 KISS-Health Project: Knowledge Intensive Social Services for Health 12 2.2 Developmental Disorders . . . 14
2.2.1 Developmental Coordination Disorder . . . 14
2.2.2 Cerebral Palsy . . . 16
2.2.3 Autism Spectrum Disorders . . . 18
2.3 Therapeutic Approaches for Children with Developmental Disorders . . . 19
2.3.1 Open Issues in the Management of Developmental Disorders . . . 21
2.4 Emerging Approaches in Neuro Motor Rehabilitation in Childhood . . . 23
2.4.1 Virtual Reality . . . 23
2.4.2 Wearable Haptic Interfaces . . . 26
2.4.3 Human Motion Analysis . . . 31
2.4.4 The Introduction of ”Serious Games” Concept Idea . . . 35
2.4.5 Open Issues in the Application of Serious Games to Developmental Disorders . . . 49
3 The Role of Educational Technology in Childhood 51 3.1 PoSE: PoStural Education in school . . . 52
3.1.1 Experimental Procedure . . . 53
3.1.2 Experimental Results . . . 57
3.1.3 Discussion . . . 61
3.2 Socio-Economic Impact Analysis . . . 62
3.2.1 Experimental Procedure . . . 65
3.2.2 Experimental Results . . . 65
3.2.3 Discussion . . . 68
3.3 Social Body Awareness in ASD Children: A Proof of Concept . . . 70
3.3.1 Concept Idea and System Architecture . . . 71
3.3.2 Experimental Procedure . . . 75
3.3.3 Experimental Results . . . 76
4 Neuro Motor Rehabilitation in Developmental Disorders 79
4.1 Concept Idea and System Requirements . . . 79
4.2 Neuro Motor Rehabilitation System . . . 81
4.2.1 Serious Games for Upper Limb Therapy . . . 81
4.2.2 Training Serious Games . . . 92
4.2.3 Multi-sensory Feedback . . . 93
4.2.4 Real-Time Motion Tracking and Dynamic Simulation . . . 94
4.2.5 Graphical User Interface . . . 99
5 Serious Games in Rehabilitation for Developmental Disorders : a Proof of Con-cept 102 5.1 Experimental Procedure . . . 102
5.1.1 Training Rehabilitation Session . . . 104
5.2 Experimental Results . . . 105
5.3 Discussion . . . 111
6 Serious Games in Rehabilitation for Developmental Disorders : A Randomized Controlled Single-Blind Crossover Clinical Trial 112 6.1 Experimental Procedures . . . 113
6.1.1 Description of the Clinical Protocol . . . 113
6.1.2 Clinical Measures for the Upper Extremity . . . 116
6.1.3 Kinematic Upper Limb Metrics . . . 117
6.2 Experimental Results . . . 119
6.2.1 Baseline Results . . . 119
6.3 Discussion . . . 144
7 Conclusion 148 7.1 Summary of Thesis Achievements . . . 148
7.2 Applications . . . 154
7.3 Future Work . . . 154
APPENDICES 156 A 156 A.1 Melbourne Assessment for unilateral upper limb function (MA2) . . . 156
A.2 Manual Ability Classification System (MACS) . . . 157
A.3 Gross Motor Function Classification System (GMFCS) . . . 158
A.4 Nine Hole Peg Test . . . 159
A.4.1 General Information . . . 159
A.4.2 Set-up (Mathiowetz et al, 1985) . . . 159
A.4.3 Patient Instructions (Mathiowetz et al, 1985) . . . 159
Bibliography 160
2.1 Main Clinical Features in SoA VR-based Intervention for Rehabilitation of
Children with Neuro Motor Impairments. . . 38
2.2 Summary of SoA in VR-based Intervention in Rehabilitation with Children with DD. . . 43
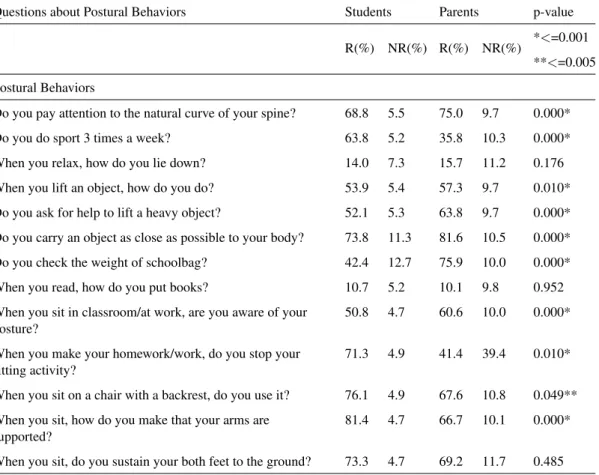
3.1 Comparison of personalized good back posture principles between students and their parents (Fisher’s exact Test) . . . 58
3.2 Comparison of the number of students with good back posture principle grouped by class grades (Fisher’s exact Test) . . . 58
3.3 Semi structured interviews to health professionals . . . 65
3.4 Participant’s self-assessment through classic questionnaire of 1-5 Likert Scale. . 76
5.1 Summary Description of Patient Group Characteristics . . . 103
5.2 One-way ANOVA: Post-Hoc Analysis (Tukey) . . . 106
5.3 Measured metrics for the Moneybox Game and for the Labyrinth Game. . . 109
6.1 Characteristics of Children Enrolled in the Study. . . 114
6.2 Metrics obtained from end-point (hand) kinematic data. . . 118
6.3 Summary of Clinical Scale Scores for all the Children with Developmental Disorders and the Randomization Result. . . 120
velopmental Disorders Groups and Results of the Baseline Measurement Com-parison Between the Groups of the Upper Limb Kinematics in All Children (Mean(Standard Deviation))). . . 122
6.5 Characteristics of the Subjects Included in the SG and C Groups and Results
of the Baseline Measurement Comparison Between the Groups of the Upper Limb Kinematics in All Children (Mean(SD)). . . 123
6.6 Results of the kinematic metrics measured in the Labyrinth and Moneybox
games for the AD, TD and SG Group (Mean(SD)). . . 124
6.7 Summary of Clinical and Kinematic Assessment of Child P7. . . 137
6.8 Summary of Main Effect of Nine Hole Peg Test, Serious Game aided Therapy
(SG) and Conventional Therapy (C) reported as Mean Value of the Difference
among Pre-Post Treatments (Mean(SD)). . . 141
A.1 Melbourne Assessment for unilateral upper limb function (MA2) [3]. . . 156
A.2 Description of Manual Ability Classification System (MACS) [4] . . . 157
A.3 Description of gross motor function for children aged 6 to 12 years by Gross Motor Function Classification System (GMFCS level) [5] . . . 158
1.1 Developmental Stages of Infants and Children [6] . . . 2
1.2 The International Classification of Functioning, Disability and Health for Chil-dren and Youth (ICF-CY) derived from the International Classification of Func-tioning, Disability and Health (ICF) ([7]) and is designed to record the charac-teristics of the developing child and the influence of its surrounding environment. 3 1.3 Conceptual Framework of Innovation in Rehabilitation. . . 5
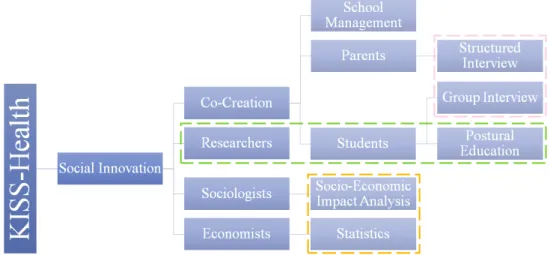
2.1 Connection scheme of the Social Innovation Strategy adopted in the KISS-Health Project for Educational Purposes. . . 13
2.2 Main area of Developmental Delay in Childhood. . . 14
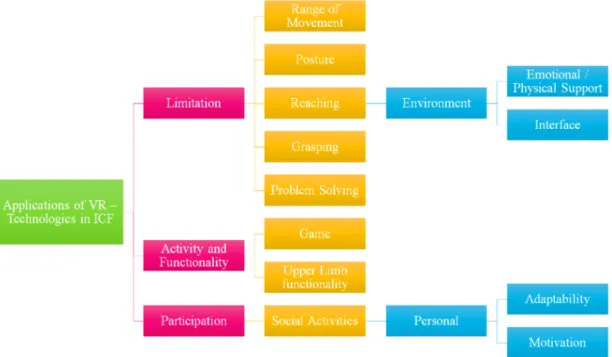
2.3 The potential application of VR in relation to ICF-CY. . . 24
2.4 Recent cutaneous devices developed in literature. . . 26
2.5 The proposed device for rendering skin stretch at the fingertip . . . 27
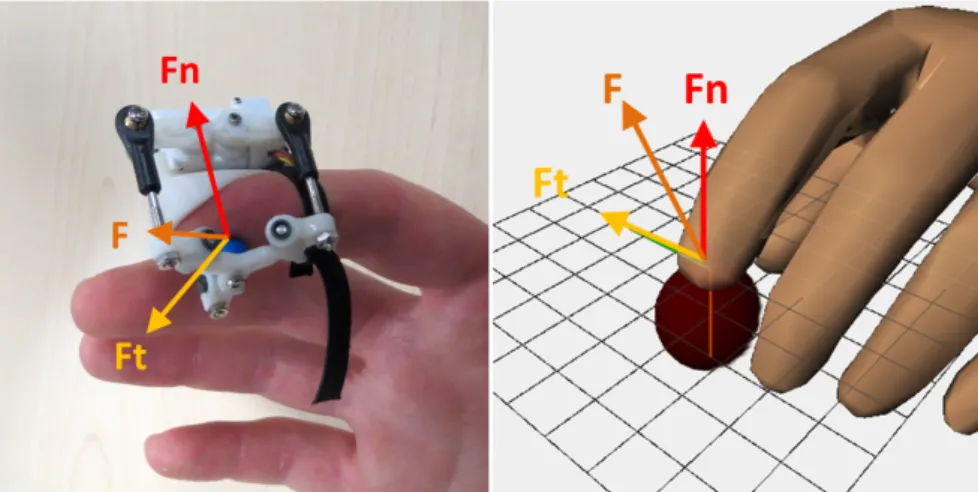
2.6 The 3 DoF fingertip haptic device rendering a generic contact force vector with both normal and tangential components . . . 28
2.7 Measured force corresponding to a normal indentation and lateral stretch of 1.5 mm. Figure (a): 3 DoF force measurement in cartesian space for one represen-tative subject. Figure (b): force-displacement characteristic for each direction and for each subject. Orange lines represent the linear fit for each subject . . . 29
2.8 Experimental setup: the computer screen, the position tracking system, the
wearable haptic devices for thumb and index fingers. . . 30
2.9 Experimental setup of the lift-and-hold experiment. Orientation of the hand
was held constant during the task. Vertical line in the VR represents the virtual prismatic guide; horizontal line represents the height threshold the cube had to
be lifted above. . . 31
2.10 Illustration of Leonardo Da Vinci’s Table on Anatomy. . . 32
2.11 Illustration of Borelli’s studies on forces and equilibiurm of the human body. . 32
2.12 ”Animal Locomotion” . . . 33
2.13 3D Tracking during Gait Analysis Processing in BTS Smart Clinic environ-ment: infrared cameras (orange), force platforms (magenta), biomechanical
model (red segments), calibrated volume (green parallelepiped). . . 34
3.1 Virtual reconstruction of the PoSE Scenario . . . 54
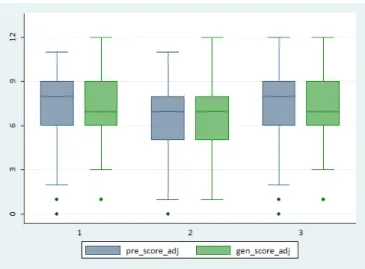
3.2 Box-plot of Postural Behaviors’ Scores of Students and their Parents stratified
by Grades . . . 59
3.3 Box-plot of Postural Behaviors’ Scores of Students and their Parents stratified
by Grades . . . 59
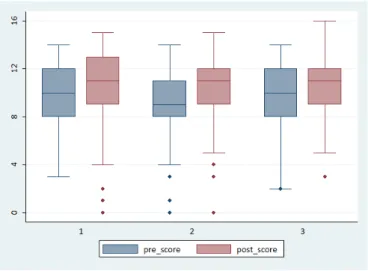
3.4 Box-plot of Pre and Post Postural Behaviors’ Scores of students stratified by
Grades . . . 60
3.5 Histogram of Pre and Post Postural Behaviors’ Mean Scores of students
strati-fied by Grades . . . 60
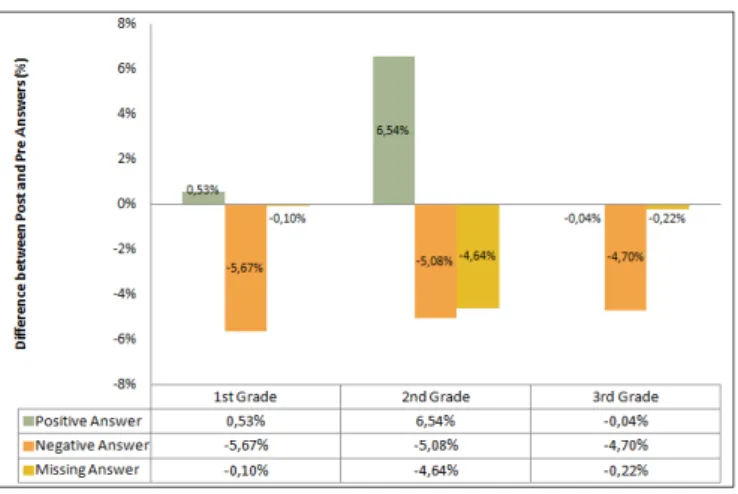
3.6 Histogram of the Trend of Pre and Post Postural Behaviors’ Answers of
stu-dents stratified by Grades (%) . . . 61
3.7 Child, robot and therapist/parents interaction. . . 72
3.9 An overview of the proposed scenario promoting a triadic interaction: the child, the therapist and the robot are involved in the session to both learn the required
skills and generalize them to the people around him/her. . . 75
4.1 Experimental Set Up: the child wears the HMD - with a detail of the projected virtual environment - and the two haptic devices. . . 80
4.2 The logic flow implemented for the two Serious Games. . . 82
4.3 Screenshot of the VE for the Moneybox Game . . . 83
4.4 Screenshot of the VE for the Marble Labyrinth Game . . . 88
4.5 A screensht of the Main GUI that allow the therapist to move among the SGs. . 99
4.6 GUI Form for Monevbox Game: the interface consists of five parts (patient information (orange square), device settings (blue square), game parameters (green square), start/stop buttons (yellow square) and information display (grey square)) . . . 101
5.1 A sequence of the experimental setup showing a CP patient performing a grasping-reaching exercise within the immersive virtual environment. . . 107
5.2 Labyrinth Game: comparison between DD (red dots) and TDC (blue stars) trajectories during contralateral movement. . . 108
5.3 Moneybox Game: comparison between DD (red dots) and TDC (blue dots) trajectories during reaching, grasping and releasing movements with the detail of velocity vectors along the path (arrows). . . 108
5.4 Measured metrics of the Labyrinth game [a] and of the Moneybx game [b] averaged over subjects of the AD, CP/DD and TD groups. . . 110
6.1 Detailed overview of the 2x2 crossover design: 2-sequence, 2-period, 2-treatment crossover design, with sequences AB and BA; a lengthy washout period was also introduced to avoid bias. . . 115
6.2 Bar plot of the mean value for RMSE, Hand Path Ratio and Smoothness in TD and CP/DD children during linear trajectory following. . . 120
6.3 Bar plot of the mean value for Movement Time, RMSE, Hand Path Ratio and Smoothness in TD and CP/DD children during the reaching task (pronation-supination movement). . . 121
6.4 Bar plot of the mean value for Movement Time, Hand Path Ratio and Mean
Ve-locity in TD and CP/DD children during the reaching task (supination-pronation movement). . . 124
6.5 Bar plot of the mean values for all the computed parameters during Marble
Labyrinth Training for the AD, TD and SG Group. . . 125
6.6 Bar plot of the mean values for all the computed parameters during Moneybox
Training for the AD, TD and SG Group. . . 125
6.7 Mean and Standard Deviation of Time Scores in Nine Hole Peg Test for
Dom-inant/Non Dominant Hand in all the four assessments (T0: baseline, T1:
post-first intervention, T2: washout, T3: post-second intervention). . . 127
6.8 Mean and Standard Deviation of Index of Performance in Linear Trajectory
Following in all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). . . 129
6.9 Mean and Standard Deviation of Index of Performance during the
Reach-to-Grasp task in all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). . . 130
6.10 Mean and Standard Deviation of Index of Efficiency in Linear Trajectory Fol-lowing in all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). . . 131
6.11 Mean and Standard Deviation of Index of Efficiency during the Reach-to-Grasp task in all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). . . 133
6.12 Mean and Standard Deviation of Smoothness in Linear Trajectory Following in all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). . . 134
all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). . . 136
6.14 Mean and Standard Deviation of Index of Performance during the Linear Tra-jectory Following and the Reach-to-Grasp task in all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). 138
6.15 Mean and Standard Deviation of Index of Efficiency during the Linear Trajec-tory Following and the Reach-to-Grasp task in all the four assessments (T0: baseline, T1: post-first intervention, T2: washout, T3: post-second intervention). 139
6.16 Mean and Standard Deviation of Smoothness during the Linear Trajectory Fol-lowing and the Reach-to-Grasp task in all the four assessments (T0: baseline,
T1: post-first intervention, T2: washout, T3: post-second intervention). . . 140
6.17 Bar Plot of the Response to Serious Game and Conventional Therapy in terms of Mean and Standard Deviation of the Time Score Difference among the Pre-Post Intervention in all the enrolled children (the sequence and the period of therapy administration was not considered). . . 142
6.18 Bar Plot of the Response to Serious Game and Conventional Therapy in terms of Mean and Standard Deviation of the Kinematic Index Difference for Linear Trajectory Following among the Pre-Post Intervention in all the enrolled chil-dren (the sequence and the period of therapy administration was not considered).142
6.19 Bar Plot of the Response to Serious Game and Conventional Therapy in terms of Mean and Standard Deviation of the Kinematic Index Difference for Reach-to-Grasp task among the Pre-Post Intervention in all the enrolled children (the
sequence and the period of therapy administration was not considered). . . 143
Introduction
1.1
Motivation and Objectives
Child development is typically defined as a normal progression by which children change as they grow older by acquiring and refining knowledge, behaviors, and skills [8]. Children de-velop skills in five main areas of dede-velopment:
• Cognitive Development: This is the child’s ability to learn and solve problems. For example, this includes a two-month-old baby learning to explore the environment with hands or eyes or a five-year-old learning how to do simple math problems.
• Social and Emotional Development: This is the child’s ability to interact with others, including helping themselves and self-control. Examples of this type of development would include: a six-week-old baby smiling, a ten-month-old baby waving bye-bye, or a five-year-old boy knowing how to take turns in games at school.
• Speech and Language Development: This is the child’s ability to both understand and use language. For example, this includes a 12-month-old baby saying his first words, a two-year-old naming parts of her body, or a five-year-old learning to say ”feet” instead of ”foots”.
• Fine Motor Skill Development: This is the child’s ability to use small muscles, specifi-cally their hands and fingers, to pick up small objects, hold a spoon, turn pages in a book,
or use a crayon to draw.
• Gross Motor Skill Development: This is the child’s ability to use large muscles. For example, a six-month-old baby learns how to sit up with some support, a 12-month-old baby learns to pull up to a stand holding onto furniture, and a five-year-old learns to skip.
Figure 1.1: Developmental Stages of Infants and Children [6]
It should be recognized that children play an active role in the development of their own skills [9] and their progress is also influenced by interactions within their environment [10]. Each child is an individual and may meet developmental milestones a little earlier or later than his peers. However, there are definitely blocks of time when most children will meet a milestone. The understanding of disability and who people with disabilities are has evolved considerably over time. The International Classification of Functioning, Disability and Health: Children and Youth Version (ICF-CY) regards disability as neither purely biological nor social but instead the interaction between health conditions and environmental and personal factors (Fig. 1.2) [11].
Figure 1.2: The International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) derived from the International Classification of Functioning, Disability and Health (ICF) ([7]) and is designed to record the characteristics of the developing child and the influence of its surrounding environment.
Disability can occur at three levels:
• an impairment in body function or structure;
• a limitation in activity, such as the inability to read or move around;
• a restriction in participation, such as exclusion from school.
The Committee on the Rights of Persons with Disabilities (CRPD) states that persons with disabilities include those who have long-term physical, mental, intellectual or sensory impair-ments which in interaction with various barriers may hinder their full and effective
participa-tion in society on an equal basis with others[12]. WHO and the World Bank estimate that more
than a billion people live with some form of disability, which equates to approximately 15% of the worlds population [13]. Among these, between 110 million (2.2%) and 190 million (3.8%) adults have very significant difficulties in functioning [13]. There are currently no reliable and representative estimates based on actual measurement of the number of children with disabili-ties [13, 14]. Existing prevalence estimates of childhood disability vary considerably because of differences in definitions and the wide range of methodologies and measurement instruments
adopted [13, 15]. As a result many children with disabilities may neither be identified nor re-ceive needed services [13]. A comprehensive approach is required for appropriate care and support including: early identification; assessment and early intervention planning; provision of services; and monitoring and evaluation. A life-cycle approach to programming provides a helpful framework to identify priority and sustainable interventions during the early childhood stage and to ensure a continuum of quality care, health services, protection and education as a child transitions from birth into and through the first grades of primary school [13, 16].
New digital technologies afford an exciting means of engaging children in therapy and provid-ing intervention environments and experiences that can easily be adapted to individual needs [17]. Play is an innate activity that enables humans to learn and grow. Despite the large variety of games, most share a number of features such as rules, competition, and interactivity with fun being the most important game element. Based on these characteristics, the video game industry is constantly evolving with video games using computers and other electronic means to support the game process while retaining the same principles but with a more modern inter-face. Novel wearable haptic interfaces has been developed during the research conducted under the framework of European Project WEARHAP ”WEARable HAPtics for humans and robots” (Grant Agreement n. 601165) with the idea of establish a novel concept for the systematic exploration of haptics in advanced cognitive systems and robotics that will redefine the way humans will cooperate with robots. Research findings derived from those studies have been integrated to address the scientific and technological challenges imposed in creating effective wearable haptic interaction [18–21].
The main objective of the present work was to identify an ideal framework for rehabilitation of children during their development. We considered the child and his/her progress as the central core for innovation in technology process and we highlighted the attention on the com-prehensive approach hoped by the WHO. We started from the consideration that health care organizations serve five distinct purposes treatment, diagnosis, prevention, education and re-search (Fig. 1.3). In serving these purposes, health care organizations must effectively manage quality, costs, safety, efficiency and outcomes. Overall, the needs of patients and the health care practitioners and providers who deliver care are the real core of the innovation process. When successful innovation were introduced, they should focus on patient’s needs, outcomes
and expectations.
Figure 1.3: Conceptual Framework of Innovation in Rehabilitation.
To address the desired purposes, we defined our framework as:
• ”Socially-Oriented”, since it dealt with social issues (inclusion, sustainability and inno-vation) of frail population (children during developmental ages);
• ”Technology” driven, since new emerging digital technologies would be introduced to engage children in early diagnosis and therapy adapted to individual needs.
Complementary objective was the design and the implementation of educational scenarios where technology and information were provided to children and their caregivers in order to promote body consciousness. Additional objective was to highlight the enabling nature, the versatility and the potential of WEARHAP. Experiments were conducted in order to test the performance of novel wearable haptic interfaces while displaying both interaction forces by skin deformation in 3-DoF and contact - no contact transition. We then integrated the cited devices in an immersive virtual environment for health application scenario. Although com-mercial motion interactive games have become more widespread, the interest in using these games in rehabilitation of children with motor disorders has increased among both clinical
professionals and parents to these children. It is not unusual that pediatric rehabilitation clinics consider to, or already have started to use these systems in their activities. Perhaps the main reason for this interest is that games may provide an opportunity to create fun and motivational forms of exercise. However, there is the need to standardize procedure and to translate it into clinical practice. A tailored serious games was realized to support a therapeutic session with children with developmental disorders. We created an immersive virtual environment with spe-cific motor task requirements for upper limb in both horizontal and frontal plane of the body and we provided accurate and congruent cutaneous feedback to the impaired hand through wearable haptic devices. Moreover, another objective of the work was to plan a Phase II pilot study in order to evaluate the efficacy of the proposed approach in neuro-rehabilitation ses-sions and potentially overcome the issues arising from the lack of efficient technology transfer in health care sector.
1.2
Contributions
With the purpose of achieving the objectives above, the presented work provided the following contributions.
The first part of the present work has been developed in collaboration with ISBEM S.C.p.A. (Is-tituto Scientifico Biomedico Euro Mediterraneo), a small research institute in the South of Italy, where I had the opportunity to successfully carry on a three-year research project, the KISS-Health (Knowledge Intensive Social Services for KISS-Health). The project was a Social Innovation program, started in 2012 and co-founded by the Italian Ministry of Education University and Research (MIUR) under the Framework ”Smart Cities and Communities and Social Innova-tion” (Grant Agreement n. PON04a3 00097). An innovative model for school-based postural education project (PoSE) to promote healthy behaviors among middle school students and their families and to moderate postural diseases was investigated, consisting in interactive lessons on back posture and good principles both in class and at home. A participatory approach was used to evaluate attempts to involve all who have a stake in outcomes in order to take action and effect change. The strength of the participatory approach used in this study relied in the contribution to empowerment social changes.
As briefly described above, the paradigm shift adopted in WEARHAP enabled novel forms of human intention recognition through haptic signals and novel forms of communication and co-operation between humans and robots. In particular, the present work proposed an application in health care scenario and in particular, we explored the integration of such wearable haptic in-terfaces in a virtual environment for the rendering of cutaneous feedback during VR-interaction as additional cues for sensorimotor integration in children with developmental disorders.We developed a Neuro Motor Rehabiliation System that could cover the specific requirements for children as formulated by therapists regarding arm anthropometry, joint range of motion and workspace, operability, safety, movement feedback, and the patients motivation. The proposed system was equipped to provide exercises for both cognitive and motor skills, but most im-portantly, it provided a positive setting for practice, by harnessing the advantages of VR to promote play, pleasure, and motivation. We implemented a highly immersive, multi-sensory virtual experience where visual, tactile and auditory feedback were congruently provided -with a defined logic work flow in order to arise children engagement during therapy while contemporary focusing their attention on the correct task execution.
A Phase II pilot study was carried on to test the efficacy of the serious games in immersive virtual environment with the support of wearable haptic devices in a real clinical therapeutic scenario. We chose a randomized, controlled, single-blind, crossover trial as clinical design since we believed it has several advantages, such as the reduction of the sample size, the study of individual participant response to treatment and participant-by-treatment interactions, the possibility for all the potential participants (in our case, children) to receive innovative treat-ments in healthcare. The clinical trial has received the approval by both the Regional Paediatric Ethical Committee (CEPR) and the Italian Ministry of Health and it is currently on-going. We will also investigate the reliability of the Neuro Motor Rehabilitation System as additional ther-apy to be delivered at home in combination with the conventional treatment according to the results achieved.
1.3
Statement of Originality
This is to certify that to the best of my knowledge, the content of this thesis is my own work. This thesis has not been submitted for any degree or other purposes.
I certify that the intellectual content of this thesis is the product of my own work and that all the assistance received in preparing this thesis and sources have been acknowledged.
1.4
Publications
A list of the publications is here enclosed:
• Conference
1. Bortone, Ilaria, Leonardis, Daniele, Solazzi, Massimiliano, Procopio, Caterina, Crecchi, Alessandra, Bonfiglio, Luca, & Frisoli, Antonio. Integration of Serious Games and Wearable Haptic Interfaces for Neuro Rehabilitation of Children with
Movement Disorders: a Feasibility Study. In 15th International COnference on
Rehabilitation Robotics (ICORR), 2017 IEEE (oral presentation).
2. Bortone, Ilaria, Leonardis, Daniele, Solazzi, Massimiliano, Procopio, Caterina, Crecchi, Alessandra, Briscese, Lucia, Andre, Paolo, Bonfiglio, Luca, & Frisoli, Antonio. (2017). Serious Game and Wearable Haptic Devices for Neuro Motor Rehabilitation of Children with Cerebral Palsy. In Converging Clinical and Engi-neering Research on Neurorehabilitation II (pp. 443-447). Springer International Publishing.
3. Leonardis, Daniele, Solazzi, Massimiliano, Bortone, Ilaria, & Frisoli, Antonio. (2015, June). A wearable fingertip haptic device with 3 DoF asymmetric 3-RSR kinematics. In World Haptics Conference (WHC), 2015 IEEE (pp. 388-393). IEEE.
4. Bortone, Ilaria, Palestra, Giuseppe, Argentiero, Alberto, Agnello, Nadia, Santo Sabato, Stefano, Bucciero, Alberto, & Frisoli, Antonio. (2015, October). STAY:
An Innovative Tool for Assessing Postural Disorders with Microsoft Kinect. In XVI Congresso Nazionale SIAMOC (poster)
5. Bortone, Ilaria, Gaballo, Giuseppe, Frisoli, Antonio, Distante, Alessandro, & Ben-venuto, Marco. (2015, May). Postural Education at School (PoSE): An innovative co-creative approach for health value. In R&D Management Conference 2015 (pp. 41).
6. Palestra, Giuseppe, Bortone, Ilaria, Cazzato, Dario, Adamo, Francesco, Argentiero, Alberto, Agnello, Nadia, & Distante, Cosimo. (2014). Social Robots in Postural Education: A New Approach to Address Body Consciousness in ASD Children. In Social Robotics (pp. 290-299). Springer International Publishing.
7. Bortone, Ilaria, Argentiero, Alberto, Agnello, Nadia, Denetto, Valentina, Neglia, Cosimo, & Benvenuto, Marco. (2014). The PoSE Project: An Innovative Approach to Promote Healthy Postures in Schoolchildren. In E-Learning, E-Education, and Online Training (pp. 49-57). Springer International Publishing.
8. Bortone, Ilaria, Argentiero, Alberto, Agnello, Nadia, Santo Sabato, Stefano, & Bucciero, Alberto. (2014, June). A two-stage approach to bring the postural assess-ment to masses: the KISS-Health Project. In Biomedical and Health Informatics (BHI), 2014 IEEE-EMBS International Conference on (pp. 371-374). IEEE.
• Journal
1. Leonardis, Daniele, Solazzi, Massimiliano, Bortone, Ilaria, & Frisoli, Antonio. (29 July 2016) A 3-RSR Haptic Wearable Device for Rendering Fingertip Contact Forces, Transactions on Haptics
2. Palestra, Giuseppe, Cazzato, Dario, Adamo, Francesco, Bortone, Ilaria, & Dis-tante, Cosimo. (22 June 2016). Assistive Robot, RGB-D Sensor and Graphical User Interface to Encourage Communication Skills in ASD Population, Journal of Medical Robotics Research
3. Bortone, Ilaria, Agnello, Nadia, Argentiero, Alberto, Denetto, Valentina, Neglia, Cosimo, Palestra, Giuseppe, & Benvenuto, Marco. (July, 2015). The PoSE Project: the Potential of Technological Learning for Postural Education in Schoolchildren.
Background and Literature
2.1
Social Innovation
During the last years, the European Commission payed more attention to the ”non-technological” aspects of innovation as they called it. DG Enterprise and Industry (Innovation Policy Unit) commissioned research in this eld. In the report the researchers recommend among other things to add indicators for organisational innovation to the European Innovation Scoreboard [22]. Several definitions have been proposed for Social Innovation according to the different pur-pose, focus and nature. Geoff Mulgan [23] identifies as one of the main characteristics of social innovation ”new ideas that work to meet pressing unmet needs and improve people’s lives”. We here proposed also the definition gave by Stanford Social Innovation Review, which stated a novel solution to a social problem that is more effective, efficient, sustainable, or just than existing solutions and for which the value created accrues primarily to society as a whole
rather than private individuals[24].
Although a precise and agreed definition of the term does not exist, social innovation ideas have increasingly been considered as a key factor in the Europe Strategy 2020, especially in healthcare, as it emerged by benchmarking in countries that have faced up this problems with the goal to identify the best practices in the field of health education at school and to evolve them in relation to our interdisciplinary approach [25]. With this evidence, the Italian Ministry of Education, University and Research (MIUR) has strived to include the younger generations
- up to the age of 30 - in the identification of social needs and the development of a culture of ”Social Innovation” in South Italy. The KISS-Health Project was cofounded under that specific institutional framework (Grant Agreement n. PON04a3 00097) focusing the attention on health problems related to postural abnormalities, actually considered one of the major problem to be addressed for their heavy economic and cultural implications.
2.1.1 KISS-Health Project: Knowledge Intensive Social Services for Health
The transition from industrial to knowledge society and the spread of sedentary lifestyle have marked a drastic reduction in physical activity with consequences on human postural attitudes. Body posture is defined as the balanced arrangement of body structures and is determined by the relative position of body segments at a given time [26].
Correct static posture is considered an important marker of health and postural abnormalities predispose individuals to musculoskeletal or neurological pathologic conditions [27, 28]. The prevalence of postural problems is associated with pain [29] and postural assessments become essential for manual therapy diagnostics, to verify and compare the efficiency of interventions. Even though Human Motion Analysis has become a well established system to support the clinicians in the evaluation process of several muscoloskeletal disorders, there are some areas, like Southern Italy, where such technological approaches are still far to be part of the health-care process. In clinical practice, specialized doctors conduct a physical exam and look for postural abnormalities depending on their abilities and experiences. Since this form of qual-itative method suffered from low sensitivity as well as low intra and inter- rater reliabilities, it became necessary for the use of standardized and validated instruments in order to ensure a more accurate, precise and systematic assessment.
The KISS-Health (Knowledge Intensive Social Services for Health) was a 3-year research project focused on an integrated approach to reduce the costs related to postural diseases for the national healthcare system . The innovative idea was the study of a qualitative and quanti-tative methodology based on the 4 Ps of Medicine (preemptive, participatory, personalized and predictive medicine). The project aimed to develop an inexpensive, practical but effective set of tools for early diagnosis, which can be considered as the first approach to postural diseases.
This massive analysis leads then to a second more accurate and clinical assessments, which will report reproducible, scientific and personalized data [30].
When dealing with studies on health in the educational field, the institutions cannot keep the subjects involved apart and they should be considered as what they actually are: the bonds of a network aiming to semantically and socially strengthen the ties. As stated by the World Health Organization (WHO), individuals have the right to claim back their own health and they must not delegate responsibility by blindly trust medical advice, because physicians need patients who are fully aware and prepared to tackle the therapies advised [7]. In order to obtain this result, the subjects involved need to understand each other and each ones needs. Full reciprocal understanding can be possible starting from a common language, easily comprehensible by all the subjects involved. For this reason, the research group has decided to adopt a socially innovative strategy (see Fig. 2.1). At the core of the concept of Social Innovation lies the active
Figure 2.1: Connection scheme of the Social Innovation Strategy adopted in the KISS-Health Project for Educational Purposes.
involvement of citizens into public service delivery. This involvement is often referred to as ”co-creation” [31]. Social innovation and co-creation are magic concepts [32], which during the last years have been embraced as new modernization or reform strategies for the public sector. Social innovation implies processes of exploration and implementation of new ideas about how a society deals, as political community, with a number of vital challenges; like the growing ageing of the population, the budgetary crises, the quality of our educational system, or the regeneration of socially and economically deprived cities and regions [33].
2.2
Developmental Disorders
Developmental Disorders (DD) are a group of conditions with onset in infancy or childhood and characterized by impairment or delay in functions related to the central nervous system mat-uration. They may affect a single area of development (e.g. specific developmental disorders of speech and language, of scholastic skills, and/or motor function) or several (e.g. pervasive developmental disorders and intellectual disability) [16]. Disorders considered neurodevelop-mental in origin, or that have neurodevelopneurodevelop-mental consequences when they occur in infancy and childhood, include:
• Motor disorders including Developmental Coordination Disorder (DCD) and stereotypic movement disorders;
• Traumatic brain injury (including congenital injuries such as those that cause Cerebral Palsy (CP));
• Autism Spectrum Disorders (ASD), such as Asperger’s syndrome;
• Attention Deficit Hyperactivity Disorder (ADHD).
Figure 2.2: Main area of Developmental Delay in Childhood.
2.2.1 Developmental Coordination Disorder
Among developmental disorders, Developmental Coordination Disorder (DCD) is one of the least studied and less understood one [34]. About 6-8% of children appear to be developing
in the usual way yet have difficulties with coordination and with learning new skills which affects their function and participation at home, at school and in the playground. DCD is the internationally accepted name for this condition. According to the Diagnostic and Statistical Manual (DSM) IV-TR, individuals with DCD have marked impairment in the acquisition and performance of coordinated motor skills given the childs chronological age and appropriate opportunities for skill acquisition [35].
Recent research has shown that the underlying reason for the movement difficulties children with DCD experience is related to atypical brain development that affects the way in which the brain forms connections (internal models) between different parts of the brain when learning a new skill. This in turn impacts on the child’s ability to use information from the senses to plan, adapt and control their movements [36]. It has further suggested that the reason of the problem for children with DCD is the deficits in the mappings from sensory to motor systems [37].
The etiology of DCD is uncertain, since it is defined as a continuous disorder and its boundaries with other continuous disorders have been questioned. One of the main comorbidity of DCD has been estimated to be ADHD with an overlap ranging between 35 and 50% of the cases [38, 39]. During the last century, the descriptions of children with motor coordination diffi-culties and clumsy movements have been largely discussed. Several authors started defining the disorder as dyspraxia referring to the constructional apraxia of the adults. However, Devel-opmental Dyspraxia (DD) [40] - as DCD - refers to a develDevel-opmental disorder, thus indicating children that appear to fail to ever acquire the ability to perform age-appropriate complex motor actions. There still exists a difficulty in medical and scientific communities in using a common terminology given its historical background [41], but DCD is the term preferred among scien-tists [42].
Perceptual modalities have been tested in children with DCD with a particular focus on motor control, involving the visual [37] and the kinesthetic modalities [43]. Proprioceptive impair-ments in localization of the tactile and double tactile stimuli have also been reported [44]. In addition, it has been argued that children with DCD having a deficit in representing actions would fail in praxic tasks and in particular in the gestural appraisal of tools and objects utli-sation. Zoia and colleagues [45] studied 35 children with DCD aged between 5 and 10 and
compared them to 105 TD children. Children were asked to produce a gesture under different conditions:
• on verbal command;
• with the tool;
• by pantomiming the use of the tool visually presented;
• by imitating the gesture performed by the experimenter.
This study was the first to report a description of developmental changes related to gestural performance. The results indicate that the proportion of correct gesture performed by children with DCD was lower than in the control group and in all 4 conditions. However, in all con-ditions the group effect decreased with age, except in the verbal command condition where in control children accuracy increased with age faster than in children with DCD. These obser-vations argue in favor of a core motor representational deficit which may be the cause of the impaired execution increasing with age. A recent review by [35] presented a detailed summary and assessed the evidence of several hypotheses for the core deficit of DCD. They suggest that impairments in two key processes in the movement circuits may be altered and have cascading effects on the movement circuits: the efference copy and the sensory feedback to estimate ac-tual body states. As such, it is possible that daily activities failed by children with DCD reflect the dysfunction of these cognitive sensori-motor components.
2.2.2 Cerebral Palsy
Cerebral Palsy (CP) is one of the most prevalent neurological disorders in children with an overall prevalence worldwide of 1.5 to 4 per 1000 live births [46]. CP describes a group of per-manent disorders of the development of movement and posture, causing activity limitations, that are attributed to non progressive disturbances that occurred in the developing fetal or in-fant brain. The main causes and risk factors of CP are: multiple birth, extreme prematurity, birth asphyxia, feeding issues, prolonged hospitalization, or postnatal infection; this disorder is more common in males [47]. Classification of CP depends on how many structures are in-volved in the damage and people with CP could be classified as having Hemiplegia, Paraplegia,
Tetraplegia, Diplegia, or Monoplegia. This classification, used in combination with the type of movement disorder (Spasticity, Dyskinesia, Ataxia, or Mixed), offers an interesting approach for clinical practice. Normally, children with CP have a combination of two or more types and functional classification procedures are recommended when a clinical decision is required [48].
The severity also determines Upper Extremity (UE) dysfunction which negatively affects chil-drens ability to perform activities of daily living and increases caregiver burdens [49]. UE dysfunction also limits childrens participation in family, school, and leisure activities: in a sur-vey conducted on 176 children, aged 58 years, with all types of CP, authors found that 63% had restricted participation in educational settings, and 57% had restricted participation in so-cial activities [50]. The activity limitations and participation restrictions were related to the severity of impairment in motor function. Thus, improving motor function in children with CP should not only improve their daily function but can also increase their participation in educational and social settings, which will lead to better opportunities for quality of life and employment as well as reduced caregiver burden [51].
CP is the most common physical disability affecting the functional development of children. Medical costs were markedly higher for children with CP and the costs were highest for chil-dren with both CP and intellectual disability. The estimated lifetime cost to care for an individ-ual with CP is nearly $ 1 million [52]. To date, there is no single agreed cure for cerebral palsy, but motor functional outcomes of affected individuals can be improved with early therapeutic intervention. Treatments for CP patients depend on the specific patients pathology and range from physical therapy to medication and surgery. When distinguishing therapeutic approaches by their main emphasis, the following basic principles can be recognized [48]:
1. emphasis on normalization of the quality of movement;
2. emphasis on functional activities, which focuses on the development of skills necessary for the performance of activities of daily living. These activities include playing, self-care activities, such as dressing, grooming, and feeding, and fine motor tasks, such as writing and drawing.
treat-ments that focus on movement [53]. The aim of the rehabilitation is to improve the patients independence in daily life activities [54]; it is during the early stages of development that fun-damental abilities and skills are developed [55] and therefore it is essential to give infants with CP an opportunity to interact with the environment for integral development (physical and cognitive).
2.2.3 Autism Spectrum Disorders
Autism Spectrum Disorders (ASDs) are behavioral syndromes caused by developmental disor-ders in the first 3 years of life, from 0 to 36 months [56]. Autism affects 1 in 68 US children [57]. One of the main feature is the difficulty of contact with the surrounding, that results in inability or difficulty in communicating with others and in complexity to maintain a functional contact with the environment. ASDs are characterized by symptoms that affect 3 main areas [58]:
1. qualitative impairment in social interaction: there are disorders of interpersonal skills with a strong tendency to isolation;
2. qualitative and quantitative impairment of social communication: verbal communication is absent or dysfunctional and it presents qualitative and quantitative disorders. Half of people with autism has a poor language and limited to few words, only a small percentage have an almost normal language characterized by pathological peculiarities: echolalia, stereotypic, prosody. The rest of the population does not reach the verbal phase;
3. behaviors, activities and interests are limited: imagination is poor, the use of objects inappropriate, ritualistic and stereotyped. To this must be added self-hetero-aggressive intent, lack of flexibility or hypersensitivity to anything that involves changes in the surrounding.
In addition to the three core symptoms of ASD, impaired movement is commonly observed in individuals with ASD. Using motion analyses, individuals with ASDs have been found to display atypical movement patterns during locomotion, reaching and aiming [59]. Research suggests that the postural system in individuals with ASD is immature and may never reach
adult levels, which can be a limiting factor on the execution of other motor skills, such as coordinated hand/head movements and inhibition of reflexes, and may constrain the ability to develop mobility and manipulatory skills.
The origin of this lack in motor coordination in ASD individuals seems to be related to the rela-tionship between Mirror Neuron System (MNS) activation, responsible of motor coordination and social skills, and the development of autism. Although differences in motor development are not considered primary diagnostic categories for ASD, researchers interested in autism are increasingly considering the importance of motor functioning of children with ASD regarding issues in diagnosis, influence on behaviors, neuropsychiatric concepts, and treatment [60]. Var-ious researchers have noted differences of gross and fine motor skills in school-aged children with ASD.
2.3
Therapeutic Approaches for Children with Developmental
Dis-orders
A review conducted on gross motor performance and self perception on children with DD showed that children in all categories (DCD, CP or ASD) displayed poor gross motor skills, although individual variability was considerable. Furthermore, poor self-concept is also a widespread phenomenon in all categories [61]. Motor disorders impact heavily on children with developmental disorders influencing their participation in daily life activities. Participa-tion is defined as involvement in a life situaParticipa-tion as part of the fulfillment of a social role. In particular, participation in leisure activities of ones own choosing is a human right and develop-mental necessity of all children, which can invoke feelings of inclusion, safety, and well-being for a child in their family, friendships, and wider society.
Children with develomental disorders face a greater number of barriers to accessing and partic-ipating in activity of daily life (ADL) than Typically Developing Children (TDC). Thus, chil-dren with DD are thus at greater risk of insufficient PA and a downward spiral of poorer motor development, psychological and health outcomes [62]. Traditionally, physical therapy plays a central role in the management of those conditions: it focuses on function, movement and
op-timal use of the child’s potential. Several approaches have been proposed over the years: from Physiotherapy to Occupational Therapy (OT) [63] to Neuro Developmental Therapy (NDT) [64] to Constraint-Induced Motor Therapy (CIMT) [65]. Here after we gave a brief description of the main concept idea for each approach and some examples of their applications in the clinical scenario [66].
PhysiotherapyPhysiotherapy mainly includes rehabilitation exercises and orthosis design. In a
systematic review of 2002, Dodd et al. concluded that training can increase strength and may improve motor activity in CP children without adverse effect [67]. The study carried on by [68] evaluated the impact of a brief physical therapy course on the motor performance of children with both DCD and ADHD. They found that 50% of treated patients reached normal MABC scores (¿15%) by the end of the therapy course, while clinical improvement without attaining normal scores was seen in a further 35%. In comparison, none of the untreated patients showed normal MABC scores by the end of the 4-week therapy period. However, the evaluation of real effectiveness of physiotherapy is still difficult since no standardized treatments or outcomes during trial have been defined.
Occupational Therapy Occupational Therapists focus on childrens occupational performance
in self-care, school, play and leisure tasks. An OT looks at the childs development, strengths and challenges in all areas of performance and determines how these difficulties affect his or her daily functioning. OTs teach the child strategies for learning new tasks, modify tasks and environments to maximize the childs abilities, and consult to teachers and parents to increase their understanding of the child. Qualitative research evidence suggests that, for many families, intervention that addresses the everyday occupations and social consequences for children with DCD is more important than the remediation of motor disabilities [69].
From a traditional physical therapy or occupational therapy training perspective, individuals with DCD and CP are trained in the most important fundamental gross motor and fine motor skills (hopping, jumping, throwing, and catching; cutting, drawing, writing), and in the basic motor abilities that are thought to be prerequisite for skills (e.g. trunk stability for certain fine-motor skills). These approaches combine underlying process-oriented approaches with direct skill training; the underlying assumptions are that motor skills are developed in a sort of
hierar-chical fashion. Basic abilities (such as postural control, in-hand manipulation, visualperceptual skills) need to be refined in conjunction with teaching complex motor skills [70].
Neuro Developmental TherapyBobath developed this method during sixties [64]. The method
focuses on the reduction of muscle tone and the inhibition of primitive and abnormal reflexes in order to facilitate the movement. In addition, the children have a greater independence and they are able to focus on the movement scheme planned by the therapist. However, intervention approaches varied among the studies, even when the interventions were derived from the same conceptual framework, thus complicating interpretation of its effectiveness [71].
Constraint-Induced Motor Therapy CIMT developed out of basic experimental psychology
research by Taub and collegues on sensory contribution to motor learning in adults disabled from stroke [65]. This therapy aims to overcome the ”learned non-use” of an extremity in hemiplegic patients by forcing the affected arm into use, immobilizing the non affected arm with a splint or sling. For children with CP, CIMT has been the subjects of many systematic reviews concluding that there is strong evidence supporting its efficacy [47, 72–74].
However, ongoing investigation is required to continue to evaluate the effectiveness of con-straint therapy in children, since there are still opened questions about which types of children would most benefit from constraint therapy; if children with different levels of upper extremity impairment respond differently; which type(s) of restraint would be most effective; what is the optimal duration of constraint therapy; is there an optimal time during a child’s development that constraint therapy would be most effective; how much therapy is needed to facilitate prac-tice of the affected arm that would most improve motor control and upper extremity function; how long should we wait before we repeat constraint therapy; what are the long term effects of constraint therapy [75].
2.3.1 Open Issues in the Management of Developmental Disorders
Early identification of developmental disorders is critical to the well-being of children and their families. A recognized clinical and research challenge in developmental disorders is the frequent lag in the diagnosis of DD, which affects the efficacy of any interventions best im-plemented early in infancy. The ability to establish the diagnosis earlier, starting in infancy,
was an agreed priority [16]. It is an integral function of the medical home approach to pro-viding primary care for children and an appropriate responsibility of all pediatric health care professionals. In addition, research studies have confirmed that parents are reliable sources of information about their childrens development [76]. Evaluating a childs development and educating families about what to expect in their childs growth, how they can promote progress, and the benefits of monitoring success, can also improve the relationship between the health care professionals and parents.
The general objective of rehabilitation interventions is to restore previous functional levels or abilities. However, when children are involved, the target level cannot be limited to re-establish a prior-value. Pediatric rehabilitation implicitly involves a moving target, the maturing child with transitory emotional, behavioral, cognitive and motor abilities. Therefore the objective in pediatric rehabilitation is two-fold, restore prior levels and facilitate the further development of these abilities [77]. Recent recommendations state that intensive rehabilitation is necessary for improving motor function in children with neuro motor impairments. These recommendations, based on motor learning theories, suggest that repetitive, goal-directed, assist-as-needed move-ments that are associated with sensory feedback and an attractive environment are likely to promote reorganization of the neuronal networks (i.e., neuroplasticity) and motor development after brain injuries or brain-based conditions [70, 78].
Physical therapy plays a central role in disease management, focusing on posture, balance, mobility, strength and function improvement. However, children find physical therapy to be mundane and monotonous when undergoing it for a longer period [79]. New strategies are needed to help promote, maintain, and rehabilitate functional capacity and thereby diminish the dedication and assistance required and the economic demands that this condition represents for the patient, caregivers, and society [80].
A major goal for therapists and special educators is to help children with neuro motor disorders in understanding the limits of the human body and help them interact in the physical environ-ment. Furthermore, a national survey of therapeutic interventions for children who have CP in the UKs National Health Service (NHS) found therapy time decreases as children age, from 12 hours per year for 06 year olds, to 7 hours for 1218 year olds [81]. Thus the necessity of
providing reliable and effective treatments.
2.4
Emerging Approaches in Neuro Motor Rehabilitation in
Child-hood
The purpose of the presented work is to investigate how Serious Games can potentially im-prove rehabilitation process in children with developmental disorders. The envised application include virtual environments, motion tracking systems and wearable haptic devices in order to create an engaging and appealing scenario, where children is fully immersed and they are able to interact with the simulated reality. The following sections presents the definition and the features of Serious Games, highlighting the attention on the interaction technologies (Virtual Reality and Wearable Haptic Interfaces) and the assessment process (Human Motion Analysis). A literature review of recent studies in this field is also presented.
2.4.1 Virtual Reality
Virtual Reality (VR) is in a broad interpretation described as an advanced form of Human-Computer Interaction (HCI) which allows the user to be part of and interact with a computer generated environment. Defining features of a VR program or application include interaction and immersion. Interaction is achieved through multiple sensory modalities that allow children to explore VEs through sight, sound, touch and sometimes even smell. Immersion is a descrip-tion of a technology, and describes the extent to which the computer displays are capable of delivering an inclusive, extensive, surrounding and vivid illusion of reality to the senses of a human participant [82]. Together, immersion and interaction contribute to sense of presence, which represents a state of consciousness, the (psychological) sense of being in the virtual en-vironment (VE) [83]. Virtual reality is a continually developing technology used to simulate an engaging environment that users experience as being comparable to the real world. The use of enriched VEs in rehabilitation was previously limited by the lack of inexpensive, easy-to-use systems that promote the easy-to-use of valid movement patterns. Development of such platforms with more user-friendly software launched a wave of potential applications for medicine and
rehabilitation [84].
VR represents one of the most innovative approach in the use of technologies for helping children improve their visual perception, motor planning and execution is the use of motion-based embodied interactive technologies [85] (Fig. 2.3).
Figure 2.3: The potential application of VR in relation to ICF-CY.
The potential of VR applications increases as revolutionary advances in the underlying VR enabling technologies develop. Rizzo et al. [86] discussed a detailed VR-specific assets avail-able and the challenges that needed to be addressed in order to promote the development of applications that could maximize the value of VR:
• The capacity to systematically deliver and control dynamic interactive 3D stimuli within an immersive environment that would be difficult to present using other means
• The capacity to create more ecologically valid assessment and rehabilitation scenarios
• The delivery of immediate performance feedback in a variety of forms and sensory modalities
• The provision of cueing stimuli or a visualization tactics designed to help guide success-ful performance to support an error-free learning approach
• The capacity for complete performance capture and the availability of a more naturalis-tic/intuitive performance record for review and analysis
• The capacity to pause assessment, treatment and training for discussion and/or integra-tion of other methods
• The design of safe testing and training environments that minimize the risks due to errors
• The capacity to improve availability of assessment and rehabilitation by persons with sensorimotor impairments via the use of adapted interface devices and tailored sensory modality presentations built into VE scenario design
• The introduction of ”gaming” features into VR rehabilitation scenarios as a way to en-hance motivation
• The integration of virtual human representations for systematic applications addressing social interaction
• The potential availability of low cost libraries of VEs that could be easily accessed by professionals
• The option for self-guided independent testing and training by clients when deemed appropriate
Virtual environments allow behaviors to be measured during challenging but safe and ecolog-ically valid tasks while control is exerted over stimulus delivery, feedback, and measurement in real time. Depending on input and display devices, VR systems can be divided into fully immersive and non-immersive setups. The advantage of fully immersive systems is the user’s strong ”sense of presence” which has been attributed to the convergence of the system’s multi-sensory input [87]. In non-immersive systems, the VR system often consists of a computer monitor, mouse, keyboard and possibly joysticks, haptic devices and force sensors. The multi-sensory illusion of actually being in the virtual environment can motivate patients to continue training over multiple therapy sessions.
2.4.2 Wearable Haptic Interfaces
Haptic devices introduce sense of touch for interaction in virtual environments and teleopera-tion applicateleopera-tions. Although most haptic devices rely on kinesthetic feedback provided to the user, other devices make use of tactile stimulation, vibrotactile or electro-tactile stimulation [88]. Also cutaneous feedback plays a relevant role in haptic perception due to the richness of mechano receptors in fingerpads [89]. Recent studies have shown how cutaneous stimuli are fundamental in recognizing shapes [90], in discrimination of curvature [91–93] and local sur-face orientation [94], in improving the illusion of presence in virtual and remote environments [95–97]. Wearable cutaneous displays exploit the above mechanisms to induce local skin de-formation at the fingerpad simulating the contact interaction with a virtual object. Different physical cues during fingerpad contact with objects are responsible for the sensory stimulation of mechano receptors, among which an important role is due to change in contact surface [98], local surface orientation [93] and skin stretch [99]. For the reasons above, a variety of different cutaneous interfaces have been devised relying on different principles of eliciting cutaneous deformation at fingerpad, see Figure 2.4.
(a) ref. [100] (b) ref. [101] (c) ref. [102]
Figure 2.4: Recent cutaneous devices developed in literature.
A class of cutaneous devices exploit the change of contact location. This aspect was originally approached in [103] with a non wearable solution. More recently [104] presented a wearable haptic device with five-bar linkage mechanism for rendering 2-DoF force feedback at the fin-gerpad: the reduction of movement to the planar case brought to significant advantages in terms of weight and bulk, but imposed strong limitations in terms of perceived feedback. Another
mean to achieve cutaneous deformation is the display of contact status and orientation through a moving contact surface. In order to improve cutaneous information with contact geometry in-formation, a first cutaneous device was developed by Frisoli et al. in [105] and then simplified in a dual finger configuration in [100], where a voice coil actuator was used to provide high speed dynamics of contact. Another simpler design was presented in [101], where simulation of tangential frictional force was limited to 1-DoF only. Similarly Pratticchizzo et al. [102] introduced a 3-DoF wearable device for cutaneous feedback based on a parallel architecture and tendon based actuation.
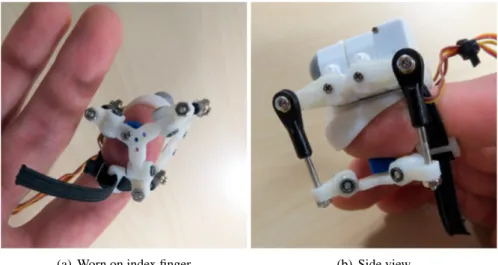
(a) Worn on index finger (b) Side view
Figure 2.5: The proposed device for rendering skin stretch at the fingertip
Skin stretch is another mechanism of local skin deformation employed to elicit force response. In [99], a simple haptic device was realized to accurately guide users through planar hand movements; more recently in [106] a 3-DoF skin stretch display was put inside the handle of a 1 point kinesthetic haptic interface. It was demonstrated that increasing speed beyond 1 mm/s the communication of stimuli did not result in significant improvement [107]. Provancher et al. [108] conducted experiments in support of the hypothesis that the addition of skin stretch to kinesthetic resistance forces increases the perceived friction magnitude. Previous results yielded difference thresholds with percent changes that ranged from 0.28 to 0.19 across friction
levels, µs= 0.2 - 0.8, respectively. The same authors found that a small amount of skin stretch
(0.27 mm) superimposed on kinesthetic resistance can have a significant effect on perceived friction [108].