Pleasecitethisarticleinpressas:FraioliMF,etal.Transsphenoidalremovalofhugepituitaryadenomaswithmarkedsuprasellarextension: Resultswithmodifiedsurgicaltechnique.ClinNeurolNeurosurg(2012),http://dx.doi.org/10.1016/j.clineuro.2012.06.019
ARTICLE IN PRESS
GModelCLINEU-3003; No.ofPages4
ClinicalNeurologyandNeurosurgeryxxx (2012) xxx–xxx
ContentslistsavailableatSciVerseScienceDirect
Clinical
Neurology
and
Neurosurgery
j o u r n al ho m e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / c l i n e u r o
Transsphenoidal
removal
of
huge
pituitary
adenomas
with
marked
suprasellar
extension:
Results
with
modified
surgical
technique
Mario
Francesco
Fraioli
a,∗,
Elisabetta
Catena
b,
Mario
Lecce
a,
Bernardo
Fraioli
aaDepartmentofNeurosciences,Neurosurgery,UniversityofRome“TorVergata”,Italy bDepartmentofInternalMedicine,UniversityofRome“TorVergata”,Italy
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received26August2011
Receivedinrevisedform1June2012 Accepted16June2012
Available online xxx Keywords: Pituitaryadenoma Transphenoidalsurgery Cerebrospinalfluidfistula Hugeadenomas
Cranialbasereconstruction
a
b
s
t
r
a
c
t
Objective:A modified transsphenoidaltechnique toremove huge pituitaryadenomaswithmarked
suprasellarextension(4.5–8cmofmaximumdiameter)ispresented.
Methods:Thetechniqueallowedtoavoidtheoccurrenceofaprecociousdescentofthesuprasellar
cister-nalplaneintothesellarplaneduringtumourremovalanditsrelatedconsequences(incompletetumour
removal,occurrenceofcerebrospinalfluidleak,prolongedtimeofpostoperativestayinhospital).
Tech-niqueisperformedopeningatthebeginningonlythelateralpartsofperitumoralduramater,leavingthe
centralpartoftheduramaterinsupportofthecentralpartoftumourandsuprasellarcisternalplane.
Afterremovaloflateralpartsofthetumour,thecentralpartofperitumoralduramaterisopenedandthe
centralintra-andsupra-sellarpartsofthetumourareremoved.
Results:Totalremovalwasaccomplishedin64%and45%ingroupstwoandonerespectively.
Intraopera-tiveCSFleakoccurredin2.4%and22.5%respectivelyingroupstwoandone.PostoperativeCSFfistuladid
notoccuringrouptwo,whileitoccurredin7.4%ofpatientsofgroupone.Averagetimeofpostoperative
stayinhospitalwas4.3and8.2daysingroupstwoandonerespectively.
Conclusion:Thepresentedmodifiedtranssphenoidalmicrosurgicaltechniqueforremovalofhuge
pitu-itaryadenomasallowedtoachievebetterresultsthanpatientsoperatedbystandardtranssphenoidal
surgery.
© 2012 Published by Elsevier B.V.
1. Introduction
Voluminouspituitaryadenomaswithmarkedsuprasellar exten-sioncanbeeffectivelytreatedbytranssphenoidalsurgery,except forrarecasesinwhichtranscranialapproach[1,2]shouldbe per-formed.
Weselected82patientsaffectedbyhugepituitaryadenomas (sized4.5–8cmofmax.diam.)withmarkedsuprasellarextension operatedfrom1997to2008.Forty-twoofthemwereoperatedby modifiedtranssphenoidaltechnique,achievingbetterresultsthan theother40operatedbystandardtechnique,concerningtumour removal,occurrenceofintraoperativedamagingofsuprasellar cis-ternalplane,postoperativerhinoliquorreaandpostoperativestay inhospital.
∗ Correspondingauthorat:DepartmentofNeurosciences,Neurosurgery, Univer-sityofRome“TorVergata”ViaOxford81,00133Roma,Italy.Tel.:+390620903057; fax:+390620903056.
E-mailaddress:[email protected](M.F.Fraioli).
2. Materialsandmethods
Outofmorethan1400pituitaryadenomasoperatedoninour Institute(byBernardoFraioli,ChiefofDepartmentofNeurosurgery, andMarioFFraioli,ProfessorofNeurosurgery,UniversityofRome “TorVergata”)from1983to2008,weselected2groupsofpatients affectedbyhugepituitaryadenomas(sized4–8.5cmofmax.diam.) withmarkedsuprasellarextension;intracavernoussinusextension waslessthan1cmofmaximumdiameterin26patients(13forboth groups).Thefirstgroupwasconstitutedby40patientsoperatedby standardmicrosurgicaltransnasosphenoidaltechniquefrom1995 to2001.Patients’agerangedfrom36 to81 years(median56.4 years).Inthesecondgroupof42patients,amodified microsurgi-caltransnasosphenoidaltechniquewasused.Patients’ageranged from32to79years(median61.3years).
2.1. Preoperativeclinicalstatus
PreoperativeclinicalstatusisreportedinTable1.Insummary, therewerenosignificantdifferencesbetweenthetwogroupsof patients.Allofthempresentedpanhypopituitarismandallneeded substitutivehormonaltherapywhichwasstartedpreoperatively in44andintheimmediatepostoperativeperiodintheother38 0303-8467/$–seefrontmatter © 2012 Published by Elsevier B.V.
Pleasecitethisarticleinpressas:FraioliMF,etal.Transsphenoidalremovalofhugepituitaryadenomaswithmarkedsuprasellarextension: Resultswithmodifiedsurgicaltechnique.ClinNeurolNeurosurg(2012),http://dx.doi.org/10.1016/j.clineuro.2012.06.019
ARTICLE IN PRESS
GModelCLINEU-3003; No.ofPages4
2 M.F.Fraiolietal./ClinicalNeurologyandNeurosurgeryxxx (2012) xxx–xxx
Table1
Clinicalpresentationofthe82ptientsaffectedbyhugepituitaryadenoma.
Subclinical hypopituitarism Clinical hypopituitarism Visualacuity impairment Visualfield impairment Suddenunilateral amaurosis Suddenbilateral amaurosis VInerve palsy Group1 9 31 40 40 2 – 3 Group2 13 29 42 42 1 1 4
patients.In22patientsbloodhormonallevelswereindicativeof
panhypopituitarismbutsymptomsweresubclinical.Threeandfour
patientsofgroups1and2respectivelypresentedapreoperative
VInervepalsy.Allpatientsbut4weresubmittedtopreoperative
oculisticevaluationandallweresubmittedtoseriated
postopera-tiveoculisticcontrolintheimmediatepostoperativeperiod,after
3,6and12months.Allpresentedseverebitemporal
hemianop-sia;moreover,allpatientspresentedvisualacuityimpairment;in
particular,in2and1patientsrespectivelyofgroup1andgroup
2,suddenunilateralamaurosisoccurredbecauseofhaemorrhagic
presentationsoftheadenoma,andtheyweretreatedbyemergency
operations.Forthesamereasoninanotherpatientofgroup2an
acutebilateralamaurosisoccurredandhewasurgentlyoperated;
inthesefourpatientspreoperativestrumentaloculisticevaluation
wasnotperformed.
2.2. Surgicaltechnique
Thesupine positionwasusedin allpatients[3].In 21 (9of
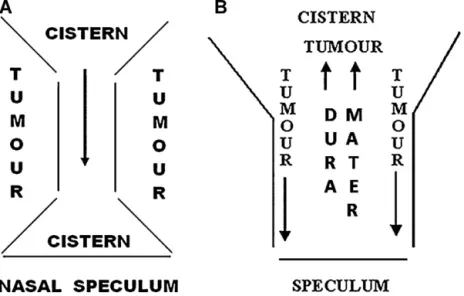
group1and12ofgroup2)themicrosurgicalapproachwas endo-scopeassisted.Themicrosurgicalendonasalsubmucosalapproach throughonenostrilwasthesameforpatientsofbothgroupsuntil theexpositionoftheperitumoralduramater.Atthispoint,aswe observedin13(32.5%)patientsofgroupone,inthesevoluminous tumours,ifsurgicalremovalstartsfromthecentralpartofthe ade-noma,thesuprasellarcisternalplanecanprecociouslydescendinto thesellaturcica,compressingportionsofthetumourtowardsthe lateralsidesoftheoperativefield(Fig.1A);therefore,thesepartsof tumourbecomedifficulttoremove,alsowiththeaidofthe endo-scope;inthiseventualityitisfrequenttheoccurrenceofdamaging thesuprasellarcisternal plane(intraoperativeCSF leak)andthe relatedpossiblecomplicationsasstretchoftheopticchiasmand postoperativerhinoliquorrhea.
Themodifiedtechniqueforthesevoluminousadenomas con-sisted in opening at the beginning only the lateral parts of peritumoralduramater(Fig.1B).Inthisway,thecentralpartof theduramaterremainsinsupportofthecentralpartoftumour andsuprasellarcisternalplane.Afterremovaloflateralpartsofthe tumour,thecentralpartofperitumoralduramaterisopenedand thecentralintra-andsupra-sellarpartsofthetumourareremoved.
3. Results
3.1. Tumoralremovalandintraoperativeprecociousemptysella Whentumourspresentedcavernoussinusextension,our pre-operativepurposewastoperformagrosstotalremoval,leaving insituthecavernouscomponentwhichwassmall(lessthan1cm diam.max.) in all patients, avoiding the risksof damagingthe intracavernousvascular andnervous structures.In group1, we achievedtotal removalin18 patients(45%),grosstotalremoval (postoperative remnantless than 1cm max.diam.)in 12 (30%) (twoprecociousintraoperativeemptysella)and6(15%)(six pre-cociousintraoperativeemptysella)patientsinwhomcavernous sinuswasrespectivelyinfiltratedornot;partialremoval (postop-erativeremnantmorethan2cmmax.diam.)wasaccomplishedin thelast4patients(10%)(intracavernous extensionin1patient)
inwhomprecociousintraoperativeemptysellaoccurred,avoiding theavailabilityofanextensiveremoval.
Ingroup2,totalremovalwasperformedin27(64%)patients, grosstotalremoval(postoperativeremnant lessthan1cmmax. diam.)in13(31%)and2(4.7%)patientsinwhomcavernoussinus wasrespectively infiltratedornot.Noprecociousintraoperative emptysellaoccurredinanypatientofthisgroup.
3.2. IntraoperativeandpostoperativeCSFfistula
Ingroup1intraoperativeCSFleakoccurredin9(22.5%)patients, andmeticulousreconstructionofthecranialbasewasnecessary. Althoughaccuracyofreconstructionofsellarpavement, postoper-ativerhinoliquorreaoccurredin3(7.5%)patients,associatedwith cephalalgiabecauseofpneumoencephalusinoneofthem.Inone patientpostoperativeCSFleakwassuccessfullytreatedbylumbar drainagemantainedfor4days;pneumoencephalusspontaneously resolvedafter5days.Inthe2otherpatients,instillationintothe sphenoidalsinusofhumanfibringlueunderCTcontrolwas suc-cessfullyperformed[4].
Ingroup2,intraoperativeCSFleakoccurredin1(2.4%)patient; nopostoperativerhinoliquorreawasobserved.
3.3. Managementofpostoperativetumoralremnantandtumoral recurrence
In group one,the 13 patientsin whomadenoma presented extensiontothecavernoussinus,weresubmittedtostereotactic radiotherapy;intheother9whopresentedatumoralremnant, asecondtranssphenoidalstage(becauseofpreviousonlypartial removal)followedbystereotactichypofractionatedradiotherapy was necessary in 3 patients, while in the other 6 stereotactic hypofractionatedradiotherapywasperformed.Notumoral recur-rencewasobservedduringanaveragefollow-upperiodof 11.2 years.Ingroup2,the13patientswithinvasionofcavernoussinus weresubmittedtostereotacticradiotherapywithoutevidenceof recurrenceafteranaveragefollow-upperiodof5.9years,whilein theother2 patientsonlyseriatedMRIs(oneatyear)were per-formed; there was no evidence of recurrence after an average follow-upperiodof4.6years.
3.4. Clinicaloutcome
Nonewneurologicaldeficitwasobservedaftersurgeryinany patientofbothgroups.In31and27patientsofgroup1and2 respec-tively,transitorydiabetes; sinsipiduswas observedand treated withdesmopressin.
OutofthesevenpatientspresentingdiplopiabecauseofVI cra-nialnervepalsy,5presentedcompleterecoveryand2othermarked improvement.
Allpatientspresentedimprovementofthepreoperativedeficit ofvisualacuityandvisualfield,includedthe4patientsofgroup oneinwhompartialremovalwasperformed.
Regardingpituitaryfunction, allpatientspresented a preop-erativehypopituitarism;inonepatientofgrouponeandanother ofgroup2a reductionofblood levelsofcortisoloccurredafter anaverageperiodof9.5yearsaftersurgery.In3and2patientsof groups1and2respectively,reductionofbloodlevelsofcortisol
Pleasecitethisarticleinpressas:FraioliMF,etal.Transsphenoidalremovalofhugepituitaryadenomaswithmarkedsuprasellarextension: Resultswithmodifiedsurgicaltechnique.ClinNeurolNeurosurg(2012),http://dx.doi.org/10.1016/j.clineuro.2012.06.019
ARTICLE IN PRESS
GModelCLINEU-3003; No.ofPages4
M.F.Fraiolietal./ClinicalNeurologyandNeurosurgeryxxx (2012) xxx–xxx 3
Fig.1.(A)Drawingofpossibleprecociousintraoperativeemptyselladuringinadequatetranssphenoidalremovalofhugepituitaryadenomas:iftumourremovalstartswith theintra-andsuprasellarcentralpartsoftheadenoma,thesuprasellarcisternalplanecanprecociouslygodownintothesellaturcicaorevensphenoidalsinus,laterally compressingpartsofthetumour,whichshouldbedifficulttoberemoved.(B)Drawingofthesurgicaltechnique.Thelateralpartsofthetumourareinitiallyremoved(long blackarrows);thecentralpartofthetumouratthebeginningisleftinsituinsupportofthecisternalplane.
Fig.2.Caseofhugepituitaryadenomawithmarkedsuprasellarextensionoperatedonbytranssphenoidalapproach.Inthiscaseasmallsuprasellarremnantwasleftinsitu becauseitwasveryadherenttosuprasellarstructures.TherewasnooccurrenceofCSFleakduringsurgery,sothatnoparticularmaterialofappositionwasputinthe operativefield,remainingfreespaceunderthesuprasellarremnant.(A)PreoperativeT1sagittalpost-contrastMRI.(B)Postoperativepost-contrastMRIperformed5days aftersurgeryshowingasmallsuprasellarremnant.Itisnoticeableahypointensityareaunderthetumoralremnant(whitearrow)representingfreespaceunderthetumoral remnant.(C)Post-contrastMRIperformed1monthaftersurgery;aninitialdescentofthetumoralremnantisevidentandthereisyetanareaofhypointensityunderthe remnantitself(whitearrow).(D)Post-contrastMRIperformed2monthsaftersurgery:anulteriordescentintothesellarplaneofthetumoralremnantisevident,withtotal decompressionofsuprasellarstructures.
Pleasecitethisarticleinpressas:FraioliMF,etal.Transsphenoidalremovalofhugepituitaryadenomaswithmarkedsuprasellarextension: Resultswithmodifiedsurgicaltechnique.ClinNeurolNeurosurg(2012),http://dx.doi.org/10.1016/j.clineuro.2012.06.019
ARTICLE IN PRESS
GModelCLINEU-3003; No.ofPages4
4 M.F.Fraiolietal./ClinicalNeurologyandNeurosurgeryxxx (2012) xxx–xxx andfreetriiodothyronine(fT3)occurredafteranaveragefollow-up
periodof7.3yearsfromradiotherapy.Patientsarefollowedwith periodicalbloodhormonallevelscontrols.
Postoperativestayinhospitalwasdifferentbetweenpatients of the two groups: an average period of 8.2 and 4.3 days for patientsofgroups1and2respectively;thedifferencewasbecause of the presence of intraoperative and postoperative CSF leak whichrequired more time ofpostoperativeobservation. Out of the three patients of group one who presented postoperative rhinoliquorrea,cephalalgiaoccurredin1ofthembecauseof pneu-moencephalus which was evident at precocious postoperative MRI;patientsofgroup2presented nosignificantpostoperative discomfort.
Nasalpackingwasremovedinthefirstpostoperativedayinall patientsbut9ofgroup1and1ofgroup2,inwhomintraoperative CSFleakoccurred:itwasremoved6daysaftertheoperation.
4. Discussion
Thepresentedmodifiedsurgicaltechniqueisindicatedforhuge pituitaryadenomaswithmarkedsuprasellarextensionoperated onbytranssphenoidalsurgery.Thetechniqueallowstoprevent theoccurrenceofaprecociousintraoperativedescentofsuprasellar cisternalplaneanditsrelatedconsequencesabovementioned,and toperformatumourremovallargerthanpatientsoperatedwith standardtechnique.
WhenintraoperativeCSF leakoccurs,the surgeonhastofill thesphenoidalsinusandthesellaturcicawithmaterialof appo-sition[5,6],andthissituationprecludes,orhoweverdelays,the progressivedescentintothesellaturcicaofthesuprasellartumoral remnant in case of gross total removal when the suprasellar tumoralremnantisadherenttosuprasellarstructures.Moreover, intraoperativeCSFleakexposespatientstotheriskofa postop-erativerhinoliquorreaanditsrelatedeventualcomplications[6] (cephalalgia,pneumoencephalus,subduralhaematoma, meningi-tis).
Onthecontrary,whenintraoperativeCSFleaksdoesnotoccur, aneventualtumoralremnantcandescendintothesellaturcica afterfewweeks(Fig.2)becauseoftheabsenceofexcessive pres-enceofmaterialofapposition.
Thetechniqueallowed,asaboveexplained,toachieveatumour removallargerthanstandardtechniqueinourpatients:evaluating attentlyourresults,excludingtumoursinfiltratingcavernoussinus (13inbothgroups)inwhichourpreoperativeplanningwastodo notremovetheverysmallintracavernouscomponentperforming agrosstotalremoval,totalremovalintheothercaseswas66.6%in group1and93.1%ingroup2.
Evaluating each singular case, the tumoral remnant can be treatedby:observationbyseriatedMRIs,executionof asecond stagedtranssphenoidalapproach[7],executionofaradiotherapic treatment [8] (hypofractioned radiotherapy or one-shot radio-surgeryinourexperience).Moreover,tumourremovalislargerin patientsinwhomprecociousemptyselladidnotoccurredthan in patientsin whom it did, as we observed in our series: 64% and45%oftotalremovalingroup2andgrouponerespectively, withabsenceofpartialremovalingroup2.Finally,preservationof suprasellarcisternalplaneallowstoremovenasalpackinginthe firstpostoperativedayanddischargepatientsafter3–5daysfrom operation.
Notwithstanding the utility of the presented technique, we retainthathazardoustractions[9]onsuprasellarremnantswhich remain adherent to suprasellar structures and which do not descend into the sellar plane during the operation, should be avoided,becausevascularordiencephalicdamagescouldoccur, whileagrosstotalremovalinthesecases(Fig.2)assuresavery importantrecoveryofpreoperativevisualdeficitsandallowsavery goodpostoperativequalityoflife.
Finally,regardingthetrigemino-cardiacreflexwhichcanoccur during transsphenoidal surgery or in generalduring skull base surgery[10,11]duetothestimulationofasensitivebranchofthe trigeminalnervewhilemanipulatingnearthecavernoussinus,we cansaythatinthepresentedpatients,duringsurgery,wedidnot observesohighandacuteheartrateandmeanarterialblood pres-surevariationstosuggestatrigemino-cardiacreflex.Itisexplicable becausewearenotuse,afterasignificantexperienceofcavernous sinussurgery[12],toovermanipulatetheeventualpara-or intra-cavernouscomponentofpituitaryadenomas,exceptforparticular casesinwhichthemaintumoralcomponentislocatedintothe cavernoussinusitself.
5. Conclusions
In our experience, the presented modified transsphenoidal microsurgicaltechniqueforremovalofhugepituitaryadenomas with marked suprasellar extension, minimizes damages tothe suprasellarcisternalplaneandthereforeintraoperativeCSF leak isveryrare;totalremovalcanbeachievedwithhigherpercentage ratethanpatientsoperatedwithstandardtechnique; postopera-tivestayinhospitalisshorterandnasalpackingcanberemovedin thefirstpostoperativeday.
References
[1]CouldwellWT.Transsphenoidalandtranscranialsurgeryforpituitary adeno-mas.JournalofNeuro-Oncology2004;69(1–3):237–56.
[2] YoussefAS,AgazziS,vanLoverenHR.Transcranialsurgeryforpituitary adeno-mas.Neurosurgery2005;57(1Suppl.):168–75.
[3]FraioliB,EspositoV,LiccardoG,GiuffrèR,CantoreG.Thesupinepositionfor transsphenoidalsurgery.NeurosurgicalReview1994;17(4):275–6. [4] FraioliB, PastoreFS,FlorisR,VagnozziR, SimonettiG,LiccardoG, etal.
Computedtomography-guidedtranssphenoidalclosureofpostsurgical cere-brospinalfluidfistula:atransmucosalneedletechnique.SurgicalNeurology 1997;48(4):409–13.
[5] KaptainGJ,KanterAS,HamiltonDK,LawsER.Managementandimplications ofintraoperativecerebrospinalfluidleakintransnasoseptaltranssphenoidal microsurgery.Neurosurgery2011;68(1Suppl.Operative):144–51.
[6]DusickJR,MattozoCA,EspositoF,KellyDF.BioGlueforpreventionof post-operativecerebrospinalfluidleaksintranssphenoidalsurgery:acaseseries. SurgicalNeurology2006;66(4):371–6.
[7]TakakuraK,TeramotoA.Managementofhugepituitaryadenomas.Acta Neu-rochirurgicaSupplement1996;65:13–5.
[8]ColinP,JoveninN,DelemerB,CaronJ,GruletH,HecartAC,etal.Treatment ofpituitaryadenomasbyfractionatedstereotacticradiotherapy:a prospec-tivestudyof110patients.InternationalJournalofRadiationOncology,Biology, Physics2005;62:333–41.
[9]FahlbuschR, HoneggerJ,PaulusW,HukW,BuchfelderM.Surgical treat-ment of cranio: experience with 168 patients. Journal of Neurosurgery 1999;90(2):237–50.
[10]SchallerB.Trigemino-cardiacreflexduringtranssphenoidalsurgeryfor pitu-itaryadenomas.ClinicalNeurologyandNeurosurgery2005;107(6):468–74. [11]SchallerBJ,FilisA,BuchfelderM.Trigemino-cardiacreflexinhumansinitiated
byperipheralstimulationduringneurosurgicalskull-baseoperations.Itsfirst description.ActaNeurochirurgica2008;150(7):715–8.
[12]FraioliB,EspositoV,SantoroA,IannettiG,GiuffrèR,CantoreG. Transmax-illosphenoidalapproachtotumorsinvadingthemedialcompartmentofthe cavernoussinus.JournalofNeurosurgery1995;82(January(1)):63–9.