DIP. DESIGN
Dottorato di ricerca in Design Coordinatore Prof. Luca Guerrini
Cycle 27
AFFECTING EMOTION THROUGH DESIGN
HOW DESIGN CAN AFFECT THE EMOTION OF WAITING TIME IN HELATHCARE CENTERS.
Supervisor I: Marco Maiocchi Supervisor II: Keiichi Sato PhD candidate: Zhabiz Shafieyoun
Acknowledgment
Firstly, I would like to give my special appreciate to my supervisor professor Marco Maiocchi for all of his positive energies to make my PhD enjoyable and thanks to his effective advice and big supports. I would also like to express my gratitude to Professor Keiichi Sato, my second supervisor, I am grateful by every thing I learned from him and his hardworking attitude, kindness and patience to encourage me throughout the process of my research. Thanks to him to accept me as a research scholar in IIT Institute of Design and gave me an opportunity to experience different academic atmosphere.
Thanks both of my supervisors for all time and effort that they dedicated to my work.
I would like to express my gratitude to my Co-coordinators Professor Trabucco and Professor Guerrini, throughout all of their support and attention in PhD plan and their special help in every step of my PhD. I sincerely thanks Simona Murina, she was kind enough to answer all of my questions immediately and make the PhD process easier.
I would like to thanks to Roberto Mazza. I highly appreciate his support during my study in Instituto nazionale dei tumori and Besta Hospital.
I have to thank my dear friend Andre Marouti for his generous effort to help me and being in my side,with positive energy and his infinity kindness.
I thanks my fellow lab-mates for the stimulating discussion and for all the fun we had in the last four years.
I am grateful to my dear friends Jerry and Steve to motivate me and encourage me to work harder for their unsparing kindness.
My thanks extend to Politechnic of Milan and the Department of Design for giving me the opportunity of studying here. Beside Special thanks to Istituto Nazionale dei Tumori, Besta, Ospedale Maggiore in Milan and San Camillo Hospital in Rome to let me to do my survey in a comfortable and supportive atmosphere.
Last but not least, I am greatly indebted to my dearest Kave. Though been far, non of this would have been possible without unconditional love, support and patience, encouragement and understanding of him.
Table of Content
Abstract
1 –
Introduction
…...…. 11.2 Statement of the problem
…...11.3 Research Aim and Objectives
…...….31.3.1 Aim
...31.3.2 Objectives
...31.4 Thesis Structure
…...32- Background and History
...52.1 Waiting Areas
.
...5
2.1.2 Interaction in Waiting area
…...…...72.2 Waiting Time
...8
2.2.1 Psychology of wait
...9
2.2.2 Factors Affecting Waiting Time
...10
2.2.3 Time Style
...12
2.2.4 Recent Solutions to Reduce Patient Perception of Time
…...122.3 Emotion
...14
2.3.1 Emotional Experience
...…..16
2.3.2 Categories of Emotion
...162.3.2.1 Categorize last emotions to the Seven Primal Emotion of Panksepp...20
2.3.3 Design and Emotion
...212.3.3.1 Sympathetic and Parasympathetic System...21
2.3.4 Scaling of Emotion
...212.3.4.1- Nonverbal Instrument (Objective – Language Independent)...21
2.3.4.1.1 GEW .…...22
2.3.4.1.2 PrEmo ...…..22
2.3.4.1.3 Emo Card…...22
2.3.4.1.4 Physiological reaction –ANS (Autonomic Nervous System)...22
2.3.4.1.4.1 Electromyography (EMG)…...22
2.3.4.1.4.2 Electrodermal Activity…...22
2.3.4.1.4.3 Skin Temperature ...22
2.3.4.1.4.4 Blood Volume Pulse (BVP)...23
2.3.4.1.4.5 Electrocardiogram (ECG)…...23 2.3.4.1.4.6 Respiration Sensor...…..23 2.3.4.1.4.7 FMRI ...…..23 2.3.4.1.4.8 PET...23 2.3.4.1.4.9 EEG...…..23 2.3.4.1.4.10 Eye Tracking ...23 2.3.4.1.4.11 Optimal Tracking...…..23 2.3.4.1.4.12 Body Tracking...…..23
2.3.4.3 Combining Verbal and Nonverbal...24
2.3.4.3.1 Kansei Engineering ...24
2.3.4.3.2 QFD...25
2.3.5 Emotional Experience
…...25
2.4 Empathy
...25
2.4.1 Empathy and Quality of Care
...262.5 Humor in Healthcare
...273. Research Methodology
.
...293.1 Ethnographic approach
...29
3.1.1 Patient stories
…...29
3.1.2 Patient in Waiting area
...31
3.1.3 Author Experience
…...…..333.2 Method and procedure: Observation
...343.3 Method and procedure: Interview
...353.4 Overview of Observation and Interview.
...…...363.5 Method and Procedure
...373.5.1 Choice of the Domain
...383.5.2 Spanning the Semantic Space
...393.5.3 Spanning the Space of Properties
...403.5.4 Synthesis
…...43
3.5.5. Results
…...43
3.5.6 Discussion
…...473.6 Flow Kansei Engineering
…...483.6.1 How can we affect the user’s emotional reactions?
...493.6.2 Entering Flow in KE process
...503.6.3 Choice of Domain
...513.6.4 Spanning the Semantic Space
...513.6.5 Spanning the space of properties
…...513.6.6 Synthesis
...513.6.7 Test of Validity
...523.6.8. Model Building step
...523.6.9 The Possible Application of the Method …...53
3.6.10 Past Experience...55
3.6.11 Conclusion...56
3.8 Summary
…...624. Conceptual Development
…...63
4.1 Hypothesis
…...63
4.2 Macro and Micro Interactions
...64
4.3 Conceptual Framework
…...65
4.4 Experience Stage Model
...66
4.5 BoneFish Analysis
...…..715. Primary Output
...726. Apply Implementation
…...747. Conclusion
…...778.Discussion
.
...79Bibliography
…...81ABSTRACT
(ENGLISH)
This study encompassed seven fundamental emotions (as defined by Jaak Panksepp) including FEAR, RAGE, GRIEF, SEEKING, CARE, PLAY and LUST (Panksepp,2012). Based on these seven emotions I have conducted a survey of 200 cancer patients using the Kansei Engineering method in 4 waiting areas in two different hospitals in Milan. Then I used Flow in Kansei Engineering called as Flow Kansei Engineering to propose Flow test. Investigating on the Effect of art in two hospitals in Milan and Rome. Moreover, I have applied a number of well-established design tools like patient journeys, scenarios, storyboards, personas and interview to complement the surveys. I have used Semantic Differential Methods in questionnaires (Osgood et al. 1969) and Factor Analysis to analyze data generated by these participants.
My analysis demonstrated how different aspects of design and social characteristics of waiting areas could influence the emotional experience of their users, and, ultimately, their perceived quality of care. For example, I verified that warm colors, abundance of light, round furniture layout and presence of art works could enhance patients’ positive emotions.
Long wait as as a problem in waiting areas was analyzed by Bonefish analysis to find the causes. I proposed a conceptual framework and a model of patient's experience to follow User Experience (UX) in Hospitals, to perform a trustable and comparable method to understand the patient’s perception of a hospital. It might have the potential to become a guideline for every waiting area and waiting time. Finally, I recommended a way of looking through waiting time in hospitals.
KEY WORD: Healthcare design, Empathy, Waiting time, Waiting area, Kansei Engineering, Emotion,
ABSTRACT
(ITALIAN)
Questo studio comprende sette emozioni fondamentali (come definito da Jaak Panksepp) tra cui PAURA, RAGE, il dolore, la curiosità, la cura, il gioco e la lussuria (Panksepp, 2012). Sulla base di questi sette emozioni ho condotto un sondaggio su 200 pazienti affetti da cancro utilizzando il metodo Kansei engineering in 4 aree di attesa in due ospedali diversi a Milano.
Poi ho usato il metodo chiamato come flusso Kansei Engineering per proporre test di flusso. Indagare sugli effetti di arte in due ospedali di Milano e Roma. Inoltre, ho applicato una serie di strumenti di progettazione consolidati come il percorso di paziente, scenari, storyboard, personaggi ed eventualmente colloqui per completare le indagini. Ho usato semantici metodi differenziali a questionari (. Osgood et al 1969) e il fattore di analisi per analizzare i dati generati da questi partecipanti.
La mia analisi dimostrano come i diversi aspetti del design e le caratteristiche sociali delle aree di attesa potrebbero influenzare l'esperienza emotiva dei loro utenti, e, in ultima analisi, la loro qualità percepita delle cure. Per esempio, ho verificato che i colori caldi, abbondanza di luce, disposizione dei mobili tondo e la presenza di opere d'arte potrebbero migliorare le emozioni positive dei pazienti. Lunga attesa come un problema nelle aree di attesa è stata analizzata mediante l'analisi Bonefish per trovare le cause. Ho proposto un quadro concettuale e un modello di esperienza del paziente di seguire User Experience (UX) negli ospedali, per eseguire un metodo affidabile e comparabile a comprendere la percezione del paziente di un ospedale. Si potrebbe avere il potenziale per diventare una linea guida per ogni zona attesa. Infine, ho raccomandato un modo di guardare attraverso il tempo di attesa negli ospedali.
Parole chiave: disegno Sanità, Empatia, tempi di attesa, Area di attesa, Kansei Engineering,
1. INTRODUCTION
1.2 Statement of the Problem
The majority of us have had at least a short journey inside a hospital for different reasons and we have come out with different experiences. All these experiences contribute to the definition of the Hospital. A Hospital is not a place just to get advice and to receive treatments from healthcare professionals but it is a place of communications and interactions among patients, staff and the environment. These three elements affect each other mentally and physically in a special situation. Paying attention to the psychological part of user's needs can help us to have a better user experience (Harris et al., 2002). Obviously, it is difficult to create a good mood in a really difficult situation, but it is not impossible. How can Design affect the atmosphere and user's emotin in waiting situations in hospitals?
A hospital is a large building with many units; in order to experiment the use of Design to impact on user experience, we can zoom in to choose one of the most stressful parts of the hospital. We believe that to find the critical part of the user's journey would be a big step to change atmosphere of the hospitals in positive way. Patient journey starts from arrival to the hospital and finishes after exit. Have a quick look in patient journey and the overall experience of the hospitals reveals that waiting area is one of the most stressful parts of the hospital. Each hospital has a variety of waits, some of them are inside waiting areas and some of them happen in corridors, in lines and in some other stops. We believe affect on the atmosphere of waiting areas can change the user experience in the whole journey. Hospital care is a part of an important relationship between patient and healthcare provider that needs
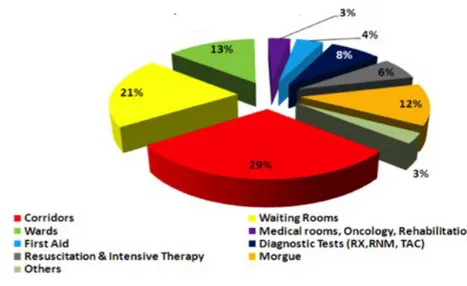
intimacy, empathy and trust. (Ancarani, Di Mauro, & Giammanco, 2009; Lin& Lin, 2010). We know that both supportive and appealing setting (place) and friendly and warm professionals (people) have the capability to affect on patient's emotion and well-being. Environmental and behavioral effect are not separable and their influence on people are undeniable. Ornella Bonimi in her study found the most stressful part of Istituto Nazionale dei Tumori (a hospital in Milan) is waiting areas. You can see her pie chart below. Corridors are a kind of informal waiting ares which get the first place and then waiting areas are in the second place (Bonomi, 2011). I later chose this hospital as a case study in my survey. Paying attention to waiting areas can help to have a positive mood in the whole Journey. This survey shows that fifty percent of the anxiety and stress is coming from waiting times. Although the character of waiting areas are different with different effects on people we can figure out how is the effect of every waiting areas in patient’s journey and compare them with each other.
Figure 1- Waiting times are one the stressful part of Instituto Nazionale del Tumori (Bonomi, 2011)
Having satisfying healthcare centers has positive effect on the society. Even it might be a prevention. To promote wellness, healthcare facilities should be designed to support patients in coping with stress. As general compass point for designers scientific research suggests that healthcare environment will support coping with stress and promote wellness if they are designed to foster: sense of control; access to social support; access to positive distraction and lack of exposure to negative distraction (Ulrich; 1991). Health theory of Salutogenesis in contrast to the Pathogenic orientation of Healthcare, suggests that we shall look for wellness factors instead of risk factors (Aaron, Antonovsky,1982). Make patient's journey easier will be a motivation for people to care their health more and do not just be in hospital when it is too late. Not only patient but also operators, nurses, doctors and their family and friends will have benefit of decreasing stress in the hospital. Decline the time of wait decrease the amount of questions about the time then reduce the amount of footwork inside the waiting areas. Changing the experience of wait will affect the whole user experience of the hospital. Emotional affect on waiting areas through design can happen by service design, interior design and behavior design. Regarding the result of our study we can choose the way of influence on patient and waiting time.
1.3 Research Aim and Objectives
The goal of this thesis is to fill the need of research, to explore: How Design affect on the emotion in waiting areas. How design has emotional impact on waiting time.
1.3.1 Aim
To affect on emotion through design in waiting areas of healthcare centers.
1.3.1.1 Objectives
How design can affect on:
Increasing positive emotion (Care, Joy).
Reduceing negative emotion (Fear, Anxiety, Stress). Increasing satisfaction with overall quality of care
Improving environmental and behavioral interaction in the waiting areas. Improving experience of wait.
Breaking icy atmosphere of the hospital.
1.4 Thesis Structure
How can I make people happy as a designer? Emotional design can be the answer to this question. Patients are a part of the society who needs special care and attention. As we know, patient's journey in a hospital is full of tension and anxiety. Applying emotional design in healthcare centers can be another answer. Hospitals are a part of healthcare centers with different units and wards. People have different goals of being in hospitals. Out Patient Department (OPD ) are some Patient who are going to visit doctors, do a test or radiography and so on in hospital and usually their journey does not last more then a day. and some patient are going to be hospitalize in hospital because of some health problems, they are In Patient Department (IPD). Observing patients in hospitals and some studies shows us the most stressful part of the hospital is waiting time (Bonomi,2012). OPD patients are usually complaining about long waits. Even IPD patients have to pass a lot of waits during their journey and they are not satisfy by that. Our focus is more on OPD patient and their waiting time in healthcare centers. Later patient means OPD patient in this study. Quality of wait has straight forward relationship with quality of care and satisfaction (Arneil, Devlin 2002).Perception of time and actual time are different in waiting areas. Patients in wait feel time is longer than real. Influence on perception of time is a way to decrease the patient dissatisfaction (Arneil, 2002).
Patient in hospital has different type of interaction with the environment and others' behavior. Environmental interactions usually are color, furniture layout, furniture, light, visual art, music, TV, magazine, computer, health information, time information, flier, brochure and nature. Physical attractions are part of interacting with environment with a big effect on patient satisfaction (Arneil, 2002, Ulrich, 1992) Behavioral interactions included other patients, nurses, caregivers, doctors, other staff, friends and family. People have a good and bad effect on each other. Feeling respect, care and comfort has a big effect on the quality of care (Waren, 1994, Waters, 1999). Behavioral effect and environmental effect have strong and direct relationship on each other (Zeisel, 1984).
satisfaction. Using physical attraction to decrease the perception of time has scored in some studies (Aneil, 2002; Dalk 2005; Ulrich 1984) such as presence and absence of a window and a view to the nature and daylight have been proven to affect on patients' emotion (Ulrich, 1984; Verderber, 1986; Wilson, 1972; Rice, Ingram, & Mizan, 2008).
Physical attraction was a key in this study to measure patient's emotion in different waiting areas with different interior designs. Measuring patient emotion in different waiting areas happen with different methods. I chose Instituto Nazionale del Tumori (INT), Besta hospital, Ospedale magiore in Milan and San Camillo Hospital in Rome for my study.
I started observing patients in hospitals during day and night for more than 300 hours. The aim of the observation was knowing patient and their feeling in waiting time. Write their stories, drawing and sketching help to know patient better. Use Likert questionnaire in Semantical differential method and Kansei Engineering in four waiting areas in two hospitals (INT and Besta in Milan) to know about patient emotion regarding different colors, furniture layouts and materials. I applied Kansei Engineering to evaluate an environment which previously, it was used to be a method for product design.
The method we chose needed some changes and add a part of positive psychology to it. I added Flow (Csikszentmihalyi, 2014) to the last method and I called it Flow Kansei Engineering with a proposal of a new survey. To know patient prefer to have useful distractions like music, pictures, paintings in waiting areas or they prefer to have health education about their disease and their treatment. Later I proposed to add flow active to the Flow Kansei Engineering to understand patient's emotion in Active Flow mode with respect to to Passive Flow mode in waiting area. New design approaches can be possible after taking the results.
Visual art as a physical attractions examined in two hospitals in San Camilo in Rome and INT in Milan. The same questionnaire based on SD methods used for this study. Participants answered questions during a painting exhibition in waiting area and they answered the same questions after the exhibition to compare their feeling during and after the exhibition in both hospitals. The result was interesting.
Macro and Micro interactions in waiting areas gave me the idea of looking at waiting time as a part of the patient journey and evaluate it inside patient journey. Based on this idea I proposed a theoretical framework of user experience in the hospital. Following patient in every step and recording their emotion reveals the overall patient emotion. Furthermore It shows in which part of the journey people are dissatisfy or less satisfy. The information let us find the most critical part of the patient journey. Innext step I am going to reframe my attempt to waiting time and user experience during waiting time to know the causes of long wait. Dividing patient journey to Flow time, Wait time and Face time and analyzing the user experience in this three parts separately and together beside analyzing the overall user experience.
The reason of Long wait was analyzed by bone fish analysis. Finding two main causes of long wait was the result of the analysis. Then I started to work on improving long waiting time by impacting on the causes of long waits.
Finally looking through the problem in different ways and all results of different studies helped me to have some assumption for improving waiting time through design. This study has a potential work in future. Moreover, I will propose a way of looking through the emotional impact on waiting time in healthcare centers to make it easy for new researchers and designers.
2.
BACKGROUND AND HISTORY
2.1 Waiting Area
The Waiting area is the most stressful part of the hospital and one of the key parts of healthcare centers, which can have a considerable impact on the experience of users attending the healthcare centers. In waiting areas patients and their families more often spend a long time without significant interactions. The perception of time in waiting areas usually is longer than reality, which can have a direct influence on the amount of stress. Attractiveness of physical environments influence the perception of time, and hence the perceived quality of care (Arneil, 2002). People expect information, care, respect, privacy and comfort in waiting areas (Waren, 1994, Waters, 1999). According to Arneil and Devlin, no studies have been carried out to inquire the effect of physical environment of doctor’s waiting rooms on patient satisfaction, nor in the perceived quality of care before 2002 (Arneil, Devlin 2002). Noise, lack of privacy, use of strange equipment, ineffective communication between patients and staff are significant part of stress factors (Winkle, 1986), which has effect on the treatment process (Ulrich, 1992). Leske talked about the fact that people in waiting time feel numb, hoping for improvement, scared or being afraid, less in control, walking around and feeling powerless (Leske, 1992). Environmental psychology helps us to know the way of changing user's emotion through Design. Zeisel says that Environment and Behavior have a straightforward effect on each other. Environment refers to the physical aspects and social characteristics of setting, where people live, work
and play. Behavior refers to the people's activities, their feelings and their thinking. How people behave might be the effect of the environment (Zeisel, 1984). Proper design of healthcare centers has been increasingly linked with improved emotional experience of users, which in turn is of prime importance for their healing process, as well as for satisfaction with the care. (Davidson, 1994; Devlin, 1992, 1995; Olsen, 1984; Ulrich,1984). Although the quality of care is a main concept in healthcare today, it is a vague one. (Arneill, 2002). According to Omachonu (1990) the quality of healthcare contains of two parts: quality in fact and quality in perception. Patients’ perceptions have a significant and deep role in their satisfaction with healthcare. Type of interactions between patients and staff, and patients and environment can make a difference for the quality of care. Ulrich believes that poor design can impact on well-being of a patient. The reasons of some negative reactions include the facts that anxiety and stress accompany illness can be due to weak design (Ulrich, 1984).
2.1.1 Physical Attraction in waiting areas
An attractive environment has effect on patient’s health, as evident throughout records of history, Florence Nightingale showed that the variety of the shapes and the brightness of the colors of an object presented to the patient had a big influence on their recovery (Dalk and Little 2005). Environmental objects include light, noise, temperature, view of nature and windows, sizes and shapes, privacy, colors, textures, furnishing layout and patterns on the wall: each of these elements can have a strong effect on patient senses. Presence and absence of a window, of a look on the nature and daylight have been proven to affect on patients' emotion. (Ulrich, 1984; Verderber, 1986; Wilson, 1972; Rice, Ingram, & Mizan, 2008). In 1984, Ulrich found that the patients who had a view to the nature through their windows, in comparison to the patients with a brick wall view, recovered sooner, and the time of their hospitalization was shorter (Arneill, 2002). Also Wilson (1972) did an experiment but for rooms with and without window and he found having a window in the room had a clear effect on decreasing delirium (Arneill, 2002). In addition, Barrington (1984) says that the connection between the ceiling and window is important too. We can regard the meaning of windows for patients as a peaceful distraction (Kaplan et al.,1972). Generally, impressions of nature have a positive effect on psychological aspects (Ulrich 1981). Arneill believes that the environment plays a phenomenal role, even more than patient and staff interaction, to transfer empathy, warmth, and friendliness (Arneill, 2002). According to Lakoff, metaphors of empathy and happiness are recognizable in all the parts of the world. People have some common signals to understand empathy, happiness and joy (Lakoff, 2014), this common language make designer's work easier. A majority of sources has been written about the environmental effects on people’s feelings. Color and illumination are two different important subjects to create pleasure. Dalk believes that the application of colors in the hospitals impact on the first impression of people (Dalk, 2005). Beside all the size of a waiting area should be large enough. That might be the reason of sitting patients usually in front of the desk to avoid to be forgotten by staff (Yoon, 2010).
2.1.2 Interaction in Waiting area
Interaction is another considerable part of the hospital. Knowing about different kind of interactions is necessary to increase positive and decrease negative emotions in waiting area in order to break the potential icy atmosphere in hospitals, and then affect on the patient’s responses. Patient in wait interact with environment and other's behavior in the same time and all make the atmosphere of waiting areas . Relationship between patient and healthcare provider has a strong effect on the atmosphere of the hospital. In the last figure patient you can see the environmental and behavioral interactions. Music, Magazine, Game, Computer are some as distraction, Visual art, light, Furniture layout, color, nature, Material and so on as physical attraction and health information and time information as patient education that patient interact with them during the waiting time. We can relate all categories of interactions to different design fields. Interior Design, Service Design and Interaction Design can affect on the emotion of users in waiting areas. Psychology helps to understand environmental and behavioral effect on waiting area.
Patient are not alone in waiting areas and they have interact with their friend or families, caregivers, nurses, other patient, doctor, operator and other staff. Their behavior has effect on patient emotion. Knowing about behavioral effect helps to think about behavior change. Behavior Design and persuasive design is another design field to influence waiting areas atmosphere.
2.2 Waiting Time
User experience in waiting time in hospitals is one of the tangible issues for most of the people
.
People interact with environment and other’s behavior in waiting areas and all these interaction make the stories of waiting areas. Waiting time refer to the time of staying in queue between entering till leaving ((Sobolev, Boris, 2008). Factors might affect time to admission can be categorized into four groups: “demands, hospital resources, waiting-list management, and patient characteristics” (Sobolev, Boris, 2008). The most frustrating element in waiting time is no control on time (Backer, 2008).Two simple aspects of waiting time are Objective time and Subjective time. Objective time (Actual time) measured by watches, clock and chronometers. The mathematical time is able to be added, multiplied and divided. This character of time can be measure an control in waiting time (Larson, 1987), and psychological cost part of objective waiting time can be decrease (Carmon, 1995). Subjective time (Perceived time) is based on experience and it is more individual. Subjective time is flexible, changeable and according to the type of activities it will be shorten or extended. How people are under or overestimate of time and how information has effect on the perception of time and the overall satisfaction (e.g.Hornik, 1984; Hui and Tse 1969; Jones and Mowen, 1991; Leclerc, Schmitt, and Dube, 1995; Taylor, 1994; Zakay and Hornik, 1991). Objective and subjective time are two world view of service providers and customers (Katz, Larson, 1991). Wait can happen before, during and after the service (Taylor,1994). Katz and Larson in 1991 proposed two ways for service provider to manage waiting, the first one is related to design a good service and the second one is effect on the customer's perception of time (Katz, Larson, 1991), still a lot of services are working in two ways. Taylor recommended a typology of waiting time based on pre-wait and during wait post-wait (Taylor, 1994).
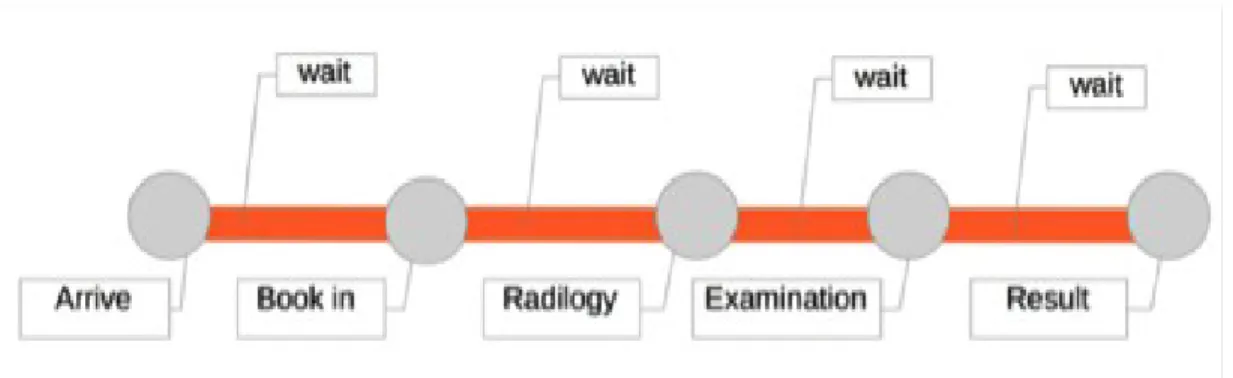
According to other studies, waiting has divided in three phases: Pre-process, In process and Post-process (Dube-Rioux, 1989). Pre-Post-process: From the time of arrival to examination. In Post-process: Time between entering and leaving examination. Post- Process: After leaving examination area tile exit. Every phases has their characters and different way to face. Another categories of wait explained by James E. and Julie K, in their study the times in hospitals divided to three separate parts: Flow time, Wait time and Face time. Flow time is the duration between arrival and registration, Wait times is the time between registration and visit the doctor or examiner; Face time is the time of spending with doctor or examiner in a office or exam room(Stahl, James E., 2011). We can say flow time is happen in Pre-process, Wait time it happen in In-process and Face time is in Post-process. Figure 2 shows the place of different waits in patient journey. Although In- process wait time has the main role on perception of time, Length and quality of face time can have a deep efficiency on quality of care and patient satisfaction (Stahl, James E., 2011). Perceived and actual waiting times are different. De Man et.al did some study in nuclear medicine and they found “perceived total waiting time is lower than the objective waiting, and perceived waiting time pre- process was considerable lower than the actual time, and perceive waiting time in process was higher than the actual time” (De Man, 2005).Sky and Miles in 1997 found the total time in waiting time was the most considerable predictor of patient satisfaction (Sky, 1997).Three phases of waiting can evaluate in two basic psychological and physiological
reactions (Taylor, 1994). Economical cost and psychological cost are paying during waiting time (Becker, 2008).“People in waiting rooms describe feeling numb, hoping for improvement, being afraid, having no control, walking around like a robot, and feeling powerless”(Yoon, JungKyoon, 2010). Beside environmental and behavioral effect on patient in waiting areas they have been effected by their characters deeply. BMC Health Service has a survey based on the relationship between patient's characteristic and their perception of time. They measured the effect on visual environment, hearing environment, body contact environment and cleanliness in different type of OPD patients in different hospitals. They found men are more satisfied than woman about cleanliness.Older patients and follow patient are more satisfied with visual and body contact environment than ew patient. Morning OPD patient are more satisfied with physical environment than After noon patient (Tsai, Chun-Yen, et al, 2007).
People with different characters has different time style. According to Usunier and Valette- Florence (1991-1994) speaking time style consisted to five dimension, “namely, economically of time, past orientation, future orientation, time submissiveness and feeling of the useless of time” (Usunier and Valette- Florence,1991-1994). This five factors has effect on:
a) Customer's reaction to delay (taylor,1990,1994)
b) Wait situation ( e.g Chebat, Filliartut, and Gelinas-Chebat,1995, Maister, 1985) c) Estimated waiting time (Hornik, 1984) , d) waiting rules (Carmon, 1995).
Agnes in university of Savoy has a study to show us the relationship between different time style and waiting experience specially in the term of passive and active patient impatience. She found time style has influence perceived time but not waiting acceptability (Durrande-Moreau,1999).
2.2.1 Psychology of wait
kraitz believes understanding patients’ concern expectation and request is a key for healthcare policy makers, researchers and clinicians to improve patient satisfaction He says satisfaction explains Satisfaction has straightforward relation with perception and expectation (Kraitz, 2001). He says the amount of satisfaction depends on the amount perception and expectation can be change, Expectation < Perception gives us Satisfaction but Expectation > Perception result will be dissatisfied. In the other hand less expectation helps better perception and satisfaction will happen.
Satisfaction = Perception – Expectation (Kraitz, 2001).
Maister (1985) talks about eight influential principles on customers’ satisfaction during waiting times. For instance occupied patients (involved in an activity during their wait) had higher satisfaction levels and lower gap compared to that of unoccupied patients (sitting idle).
“Unoccupied time feels longer than occupied time. Pre-process waits feel longer than in process waits. Anxiety makes waits seem longer.
Unexplained waits are longer than explained waits. Unfair waits are longer than equitable waits.
The more valuable the service, the longer the customer will wait. Solo waits feel longer than group waits” (Maiser, 1985).
Five necessary conditions was recommended by Rondeau to organize the waiting process: 1-Engage people
Connect new patient with old patient for sharing experience. 2-Decrease patient’s hospital related anxiety
Inform people about time, treatment process and facilities. 3- Improve communication with patient
Non-medical and medical chatting with patient. 4- Ensure quality
Make sure of equal process for every patient
5-Increase interaction between patients in waiting time.
More interaction makes people busier and they put them in groups of patients with same problems (Rondeau, 1998).
2.2.2 Factors Affecting Waiting Time
Waiting time is dealing with four difference factors, a) Customer's reaction to delay (taylor,1990,1994), b) Wait situation ( e.g Chebat, Filliartut, and Gelinas-Chebat,1995, Maister, 1985) c) Estimated waiting time (Hornik, 1984) , d) waiting rules (Carmon, 1995). Economically, time is precious and loosing time of wasting time is facing with regret of loos. “Passive impatience” happen when People have nothing to do and they just pay attention to passage of time, they feel they are in empty time and they feel lucked in this time ( James, 1946). They feel helpless and being under time pressure (Durrande-Moreau,1999). Affect on impatience and perception of time to transfer from emptiness of time called “Active impatience” (Durrande- Moreau,1999). So, waiting experience is included passive impatience represent longer waiting time and active impatience linked with shorter waiting time. Quantitative individuals time shows strong economic time mostly by looking at future and qualitative person displays low attention to economic time toward past and they prefer to live in present (Prime, 1994). Qualitative people maybe they do not care of being on time and quantitative people's plans would be disturbed by quick activities. Agnes Durrand assumption is perceived of time for quantitative people are more negative than qualitative people (Agnes Durrande- Moreau, 1999).
Although longer waiting time has a negative effect on overall satisfaction, good communication and strong relationship between patient and staff reduce the negative effect (Miceli and Wolosin, 2004). Length and experience of waiting can effect on the perception of quality of care for patients and visitors (Arneil& Devlin, 2002). The patients consider waiting as inactive, wasted or lost opportunity time. It was found patient satisfaction decreased with longer waiting times (Katz 1991, Dansky 1997). Interventions to decrease perception of wait times and increase the perception of service with paying attention patient expectations, can improve patient satisfaction (Olanrewaju, 2011). Relationship between patient and healthcare providers has a strong effect on decrease the perception of time (Anderson, 2007).
Majority of the research in this area primarily revolves around three factors: actual waiting time, perceived waiting time, and the gap between them The perceived waiting time is often different from actual waiting time (Taylor, 1994). This means identifying and improving the variables that influence the perceptions of waiting could improve patient’s perceptions regarding wait time (Stahl, James E., 2011). Reduce perceived time has a positive effect in patient satisfaction. Figure 4 was published in the Journal of Service Research in November 1999 and it is proposed a model based on actual waiting time and time style which can be passive impatience of active impatience and all influence on customer’s satisfaction. So time style has a big effect on user experience in waiting time. They used this model to understand people with different time style (actual time, economic time, past oriented and future oriented) has different experience of waiting time. People with more economic time style are more active impatience than others and no more negative. They show short waiting time dose not need information system about their wait.
Figure 4 - A proposal Model of Actual and perceived time (Durrande- Moreau,1999
2.2.3 Time Style
According to Usunier and Valette- Florence (1991-1994) speaking we as a human have different kind of time style including “Namely, Economically, Past orientation, Future orientation, Time submissiveness and Feeling of the useless of time” (Usunier and Valette- Florence,1991-1994). Namely is the real time. The economically time is precious and loosing time of wasting time is facing with regret of loos, Past and Future oriented is living in the past and future and forgeting about current time. “Time submissiveness” define a dutiful and harmonize tendency towards time indicating appointment and schedules. This is a perceptual of individual relation to time. In psychological dimension of time talks about how people cope with time and external resources it is divided to motivational aspects or time related to anxiety ( Usunier, jean-Claude, 2007). Aging has a effect on perception of time, older people being more aware of the time and more concern about the way of spending their time ( Szmigin, Carigan, 2001). Durrande- Moreau and Usunier investigated on the effect of time style on waiting experience in a service context. Quantitative people contribute to have more negative perception of waiting experience than qualitative people ( Durrande, Usunier, 1999).
2.2.4 Recent Solutions to Reduce Patient Perception of Time
The importance of relation between patient satisfaction and waiting time is reason for proposing multiple strategies to decrease wait times (Weiss, 2003).Feddock, Christopher A., et al found a relation between perception of time for patient and the role of physicians. In this survey they specified the role of spending time with physician in patient satisfaction. Patient with long wait, more than 15 min wait in waiting room or more than 10 min in exam room, dissatisfied with short time of visiting physician. According to this study physician can decrease the negative effect of waiting time by spending more time with their patients (Feddock, Christopher A., 2005). We should be considerable about interaction between patient and their physicians. Leddy says patient in long waiting time, more than 20 min are more satisfied in a comfortable and peasant waiting area (Leddy, 2003). We can see in several surveys the importance of the amount of physician time spending with patient (Dugdal,Epstein, 1999, Gross et al. 1998, Lin et al, 2001). Spending time with patient in one way and being with them in psychosocial issue in another way (Roter, 1997) beside explaining the cause of the patient’s problem (Jackson et al, 2001) or non-medical chat with them (Gross, 1998) make people more satisfy.
Heather Sherwin in 2013 has a study about waiting room “ wait”, waiting room can be a place more than just for wait. Make more interaction in waiting room between patient, caregiver, physician, doctors, operator and nurses can change passive waiting to active care. For example physician can take blood pressure of patient during their wait, or they can talk together, fill some questionnaire during waiting time, provide patients with education regarding their health, participate patient family in health questionnaire. Briefly of his speaking is “using waiting room, to screen, to monitor, and educate could enhance a patient’s primary health experience, leading to increased patient satisfaction and ownership”. (Heather N.Sherwin, 2013). BMC Health Service Research in one study showed time spend with physician has a strong effect on patient satisfaction. Reduction in Satisfaction relevant with long waiting time significantly decrease with increased time spent with physician. Above all the combination of long waiting time and have a short visit with the doctor has a very low overall patient satisfaction (Roger T, Anderson, 2007). Investment of time and money- psychological and physical should have a significant meaning. In other words, making a good combination of waiting time and visit time can increase patient satisfaction. Some variable service such as Primary care, health plan or organization can have a straight effect on patient satisfaction (Roger T, Anderson, 2007). Fabian Camacho talkes about “patient willingness” he believes waiting time is an important part of time price and willing to wait should be increased with patient perception of rising quality of care. Knowing about the amount of “Willing to wait” has effect on patient satisfaction and quality of care (Camacho, 2006).
Table 1-1- Implementation in psychology of wait
Based on mentioned recent solutions, I added one more column to the last table. Every row has an example of recent solutions to decrease the perception of time based on psychology of wait. Fill questionnaire and get feed back not only makes patient busy but also give them the feeling of respected (Heather N.Sherwin, 2013).
In process is wait time in patient journey, talking with physicians in wait time and doing prime healthcare has a good effect in In- Process(Leddy, 2003).Preparing books, flier ,brochure, movies or information on the wall help patient education. Patients with an amount of knowledge about their disease and the treatment process and side effects have less stress and they are more satisfied (Heather N.Sherwin, 2013). Informing about the time is another way to give the control of time to patients. They will feel better to count down the time to reach their time ((Gilbert, 2009). If the reason of being in the hospital is seeing a doctor and explain about their problem and make a decision about it, the most important part of the journey will be face time and increase the quality of face time will increase the quality of care and increase patient satisfaction (Stahl, James E., 2011). We have not found a study for being in a group and being alone yet.
2.3 Emotion
We need to know people's emotions in waiting time in order to be able to impact on them in a positive way. Before we should know, emotion, being in a mood and personality are three different issues. Briefly, being in a mood is longer period than emotion and personality is longer than mood (Parrot, 2000).
Emotions are complex in distinguish and categories.The definition of the term “emotion” has a long history, from more than one hundred years ago. Emotion is a multifaceted phenomenon, which includes expressive reactions, behavioral reactions, physiological reactions and subjective reactions (Desmet, 2005).
We have a variety of definitions for emotion in different fields such as psychology, neuroscience, design. You can see some of the definitions blow:
• Emotion as a word “ can be defined as a conscious mental reaction (as anger or fear) subjectively experienced as strong feeling usually directed toward a specific object and typically accompanied by physiological and behavioral changes in the body” (Merriam, 2004)
• Generally speaking, emotions are inseparable part of cognition and are the conscious experience of affect (Norman, 2007) andEmotions are indispensable part of cognition (Norman, 2005).
• Emotion” define as, “disturbance of mind; vehemence of passion, pleasing or painful”
Duchenne de Boulogne (1862) and Darwin (1872) started in the 19th century to define emotion in science. Emotion has never been statistic but by scientific approach we have had more quantitative looks on it.
Marco Maiocchi has described the process of emotion's meaning and emotions of users from every signals. The following figure is shown users have meaning and emotion of all signals by simple and complex perception within technical and cultural constrains.
Figure 5 :The Process of Emtion's Meaning From Signals (Pilan, Maiocchi, 2013)
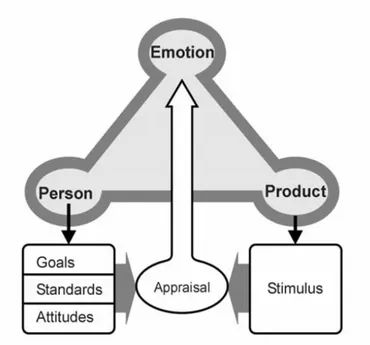
Desmet proposed a basic model of emotions that are related to human-product interactions and identified by concern, stimulus, and appraisal (Desmet, 2002). How people have emotional reaction to signals. Desmet and Hekert introduced a model of product emotion, to respond how emotions are elicited? This model is based on cognitive - functionalist view on emotions. The functionalist approach in emotions can bedescribed as “the felt tendency toward anything intuitively appraised as beneficial, or away from anything intuitively appraised as harmful” (Arnold, 1960). Based on this definition, Desmet says that “emotions pull us toward good stimuli and push us away from bad stimuli” (Desmet, 2001). They introduced product emotions based on three approaches to concern:
(1) Goals,
(2) Standards, and
(3) Attitudes (Ortony, Clore, and Collins, 1988), (Desmet, 2001).
• Goals: Three kind of goals define regarding products: utilitarian, social and hedonistic. • Standards are our expectations, patterns and conventions regarding to things.
• Attitudes are changes in our taste about like or dislike.
Figure 6- Desemet Emotional model (Desmet, 2001)
2.3.1 Emotional Experience
The definition of emotion has been changed from passion to desire. Emotions have physical and mental effect (Picard, 1997). Touch, sight and sound, taste and olfactory experiences can affect on emotional experiences and cognitive emotions. People can experience different emotions in the same situation, based on their background, their experience and their perceptions. By having a look on the history, we can see how many definitions of emotion exist. “ Emotions change behavior in a short time and quickly, moods can measure by hour or days. Traits are more longer, years or life time. A collection of traits create personality. All above mentioned factors are changeable. Multiple personalities in different groups emphasize different traits and our flexibility (Norman, 2004).
2.3.2 Categories of Emotion
A variety of emotion categories exist in different fields such as psychology, neuroscience and design excite. In the next figure we summarize different positions of some authors: a lot of scientific approaches in basic emotions are present in literature, but strongly different from each other. According to Plutchik basic emotions are acceptance, anger, anticipation, disgust, joy, fear, sadness, and surprise (Plutchik,1980). Moreover, he introduces primary, secondary, tertiary emotions.Ekman says there are six emotions: anger, disgust, fear, joy, sadness and surprise (Ekman 1999). Damasio in 2005 talked about primary and secondary emotions both producing changes in body states; but thoughts evoke the secondary emotion. The emotions that a person feels non-cognitively are primary emotions. Secondary emotions are produced cognitively (Damasio, 2005). Cannon suggests that different parts of the brain
can be related to an emotion, for example, the hypothalamus and the limbic system are joined with emotions (Oatley et al, 2006). Bodily experiences we call emotions, consist of two aspects: cognition and sensation. We know that the body is not separable form consciousness. Russell categorizes emotions in two dimensions. One is the range between pleasant and unpleasant and the other is the rang from excitement to calmness (Russell, 2003).
Figure 7- Russel emotional Model ((Russell, 2003)
Gomez believes if a negative emotion follows a positive emotion the result will be an overall of noticeably negative experience. This theory also shows that if a positive emotion followed by another positive emotions, it creates a link between positive emotions and the overall experience is positive (Gomez, 2008).Below you can see a chart of different categories of emotions. This chart was made by Ugur, Secil one of the PhD graduated of Politechnic of Milan. She worked on embodiment of emotion through wearable technology.
Figure 8- Circumflex of Basic Emotions and Theorists (Ugur, Secil, 2011).
Panksepp defines seven fundamental emotions, fear, rage , grief, seeking, care , play and lust. He says an emotion is the status deriving from the activation of specific neural circuits by a specific neurotransmitter (Panksepp, 2012). Neuroscientists believe, the human brain has three layers. The inner part (reptilian) which emotions arise in this part, mainly related to survival emotion such as seeking, fear, anger., the middle part, developed in mammals, which is related to maternal emotions, and the upper part (neocortex) is more related to rational and logic processes.
“Nothing is more complex, mysterious, and subject to conflicting theories and interpretations than human emotions” (Denzin, 2007).
· According to Panksepp speaking emotions as one of the mechanisms to increase the survival of the species; Based on his words and Darwin theory and some other studies, animal and human both feel emotion (Darwin, 1872). As we know Darwin was the pioneer of this approach.
· Panksepp considers every emotion as the activation of a specific part of the brain through a specific neurotransmitter class, and he says basic emotions are seven. He knows seeking, play and care aspositive emotions with positive- affect and fear, rage and grief as negative emotions with negative- affect.
rate, and skin conductance.
Nevertheless, the works published by Panksepp don't examine in deep the peripheral nervous system (sympathetic and parasympathetic systems, vagus nerve, etc); those aspects are handled by other authors, such as Sapolsky (Sap 2004) and Porges (Porges, 2011). People's emotion are mixing of these basic emotions, for example jealousy is mixing of seeking, lust and fear and may be grief (Panksepp 1982, 2010c) .
Seven Basic Emotions :
. SEEKING (expectancy): SEEKING trickles our look to search and find the meaning of our
surrounding beside making satisfy our primary needs such as hanger, thirst and find a shelter to protect ourselves which might leads us to discover some ideas, forecast and models. Seeking is living under the “brain award system” (Panksepp 2012). One of the most important intuitive emotional system that stimulate searching, exploring and the reason of being excited to gain the desires in creatures. SEEKING urge. “In a sense, SEEKING is the “granddaddy” of all the emotional systems. To satisfy LUST, one must seek relationships. To feel tender loving CARE, one must seek to help those who need help, especially babies. To feel full RAGE, one must seek to harm those who would take resources away from you. To respond well to FEAR, one must seek safety. To make your PANIC/ GRIEF work for you, you must seek out those who would support your needs. To PLAY with great joy, you must find friends” (Panksepp, 2012). When we are hungry, thirsty, cold or lonely, when we are scared , we care seeking for a solution to answer our needs and desires.. Seeking is a stimuli system for learning to make it an exciting experience. Seeking leads us to feel good by providing a kind of excitment. Peter Milner has called seeking “ brain reward system” (Olds & Minler, 1954). Brain dopamine is the fuel of seeking.
· RAGE (anger): Disappointed seeking, seeking with no achievement create frustration then rage, trend to quick reactions. Rage can change to jealousy and hatred. Anger can be the cause of Rage and some times it happen for protecting ourselves. Jim Averill’s (2010) definition states that “anger refers to an emotional state that involves both an attribution of blame for some perceived wrong and an impulse to correct the wrong or prevent its recurrence; aggression is an attempt to coerce another into taking, or refraining from, some action against his or her will and not for his or her own good”. Rage system can increase aggression dramatically. Many frustrations are coming from difficult times, increasing difficult time is a cause of human anger. Generally female have less anger than males. Difference in sex circulating hormones is a part of the reason of sex difference. Testosterone has influence on aggression and it is promote male dominance tendencies. Social rejections are another causes of aggression ( Panksepp, 2012)
· FEAR: leads creatures to survive, pain, threat and forbid. Freezing and flight are two objective related to Fear. Pain is fear stimulation. Becoming afraid of conditional stimulus are simply happens. Symptoms of expecting anxiety are rapid heartbeat, sweating, gastrointestinal upset, and increase muscle tension which are characterizing Fear. Experience and a memory of a fear in childhood can be a reason of fear in adulthood. Weak people like children have more fear, because they feel not having the power to resist danger. Some times children put themselves in danger like going up of a ladder that's because they still do not understand the particular danger.There is close relationship between Fear and Rage and both associated with fight responses and flight responses, both happen in a kind of danger (Panksepp, 2012).
· PANIC or Grief ( sadness): separation distress, social loss, grief, loneliness, specifically for the absence of maternal care Grief is one of the reason of depression and this is an emotion you have never wished. We can say grief is “the dark side of our capacity for love and Play”. Stress chemical arouse the grief system. Panksepp talks about new treatment of depression and he introduces it in three ways :
First, use of “ safe opioid” to reduce psychological pain and depression (in process method). Second, deep Brain Stimulation of Seeking System to evaluate capacity for enthusiasm.
Third, the genetic analysis of Play- Increase the amount of social joy in the brain to classify new neuro- chemistries to help positive social feelings.
Care can decrease the grief. When we hold a chicken in our hands and give the feeling of safe and comfortable place to it, we decrease the feeling of loneliness. Panic/ Grief might be the strongest emotional resonance to assist empathic devotion (Panksepp, 2012)
· LUST(sexual excitement) : involves sex and sexual desire; Lust linked with different homeostatic and sensory affective mechanism like other emotional system. Negative emotions such as Fear of Grief decrease sexual arousal but mild pain some times increase it. Loving relationship with sexual satisfaction seems a to be a reason of happiness and longer life. In biological level, brain's sexual organization may not match well with sociocultural identity. Furthermore, people can be in “ mismatching” bodies and minds. Males and females have different approaches to Lust and their attractions are different. Sexual desire is the reward of Seeking System and it helps to increase Dopamine ( Panksepp, 2012).
· CARE (nurturance): maternal nurturance;
Human motherhood is a miracle. The role of extending families have been changed with the passage of time. Care reduces Grief and Grief reduces Play, this is the interrelationships between Care, Grief and Play. The positive effect of Care is rising dopamin in the brain (Panksep, 2012). In fact without maternal care and psychic of Panic, empathy would not exist ( Panksepp, 1998: Watt,2007). Care can be sexual and non sexual emotional system. Oxycontin is one of the important maternal chemical (Peterson et al. 1982; Keverne & Kendrick, 1994) in more quantities in female brains than male brains (Jirkowski et al., 1988).
· PLAY (social joy) : Play, joy. Playful activities bring great joy. Panksepp says this is difficult to define Play chose the five criteria of Gordon Burghardt (2005) which summarized it in a single sentence “ “Play is repeated, incompletely functional behavior differing from more serious versions structurally, contextually, or ontogenetically, and initiated voluntarily when the animal is in a relaxed or low-stress setting” (Panksepp, 2012).
Panksepp has affective feeling for every seven primal emotions. Affective feeling of Seeking is Enthusiasm , Rage/ Pissed- off, Fear/Anxiety, Lust/ Horny, Care/ Tender & Loving, Panic/Lonely & Sad and Play/ Joyous. He is talking about them in Ted Talk and he mentioned about all in his book seperatley (Panksepp, 2012).
2.3.2.1 Categorize last emotions to the Seven Primal Emotion of Panksepp
Categorize last emotions in the last chart in a new chart (blow) based on seven basic emotions of Panksepp shows Lust is one of the emotions with no attention in other's classifications and Fear then Grief and Seeking are noticed more. It seems positive emotions from Panksepp speaking have thin columns between all other emotions. Widest column is related to Grief, it means we found more emotions under the meaning of grief to situate in this group.
Table 2- Basic Emotions Under Panksep's Category of Emotion
2.3.3 Design and Emotion
According to Norman design has three levels, Visceral, Behavioral and reflective. Each part helps to shape the experience. Visceral is about initial reactions of people to design. What nature does is Visceral. Interpretation of emotional signals of environment use in visceral level. Behavioral level is about use, with not too much attention to apprentice (Norman, 2004). Functional can introduce behavioral level which needs understanding people. Good behavioral can be the base of design. Reflective is about variety sides of design such as culture, meaning of product and message (Norman, 2004). Smith and Kirby talked about level of processing in appraisals; 1) Direct perception which dose not need the activation of mental presentation (Viscersal level). 2) Automatic response based on the background and memories outside of the consciousness ( Behavioral level). 3) Conscious reasoning ( Reflective level) (Smith and Lirby, 2001). These levels are comparable with three level of perception 1- Simple perception, 2- Complex perception and 3- metaphors (Lakoff, 2003).
Desmet says two other approaches are introduced between different appraisals, thematic and componential. The first approach is a short distribution of an overall meaning of a situation. For instance for joy overall meaning is a progress to achieve a goal (Lazarus, 1991). In the second one focus is on every steps and different aspect of situation as appraisal component ( Roseman, 2001; Scherer,2001) both approaches should be understood for designing emotion (Desmet, 2009). Desmet believes design for happiness should play with these four features of human: Talent and skills,
contribution, personal value, pleasure (Desmet, 2011). “The importance of emotion and context involved during interaction with artifacts or environments is also activated within activity theory”( Gomez, 2008)
2.3.3.1 Sympathetic and Parasympathetic System
Before start to talk about scaling of emotion, talking briefly about sympathetic and parasympathetic systems can be useful. There are two major branches in automatic nervous system. The Sympathetic and Parasympathetic. The sympathetic system evaluate for active responses such as heart rate, respiration. The Parasympathetic branch approves in passive situation such as the slow heart rate. It is also sensitive in emotional changes and it advocate, sexual arousal, salivation and tears (Panksepp, 2012).
2.3.4 Scaling of Emotion
According to Rodaway, sensation and cognition are two dimensions of perception (Rodaway, 994). Sensation is the relationship between human body and the environment with five different senses. Cognition is a mental process. Human body shows emotion in different ways in verbal and nonverbal communications. Methods have been developed to scale emotions based on their verbal and nonverbal manifestations and physiological reactions:
2.3.4.1- Nonverbal Instrument (Objective – Language Independent)
Nonverbal instruments are language independent and can be used in all cultures. In addition nonverbal instruments are more objective than subjective which is not relay on participant own assessment ( Desmet, 2005). These instrument approach a limited set of basic emotions such as fear and rage (Cacioppo et al. 2001) and the instruments can not enter to the field of measuring mixing of emotion (Desmet, 2005). Facial expression, vocal, postural expression and gesture shows emotions in nonverbal communications. Desmet presented a non-verbal self-report instrument to measure 18 positive and negative emotions specified by product design. (Desmet, 1999) Ekman found out that each emotion is associated with a particular pattern of expression (Ekman, 1994). Facial Action Coding System (FACS; Ekman & Friesen, 1978), and the Maximally Discriminative Facial Moving Coding System (MAX; Izard, 1979) are measuring facial and vocal reactions. Facial Expression Analysis Tool (FEAT; Kaiser & Wehrle, 2001) automatically codes videotaped facial actions. Vocal instruments are based on theories which are linked patterns of vocal cues to emotions (e.g. Johnstone & Scherer, 2001). These instruments measure the effects of emotion in multiple vocal cues such as average pitch, pitch changes, intensity color, speaking rate, voice quality, and articulation (Desmet, 2005).
2.3.4.1.1.GEW
Geneve Emotion Wheel is a new instrument for measuring emotional reactions to objects, events and situation. GEW is invented by Schere, Shuman, Fontain and Soriano in 2013. (sherer, 2005), (Sheresr, 2013).
2.3.4.1.2.PrEmo
The PrEmo tool is invented by Desmet (Desmet, 2005) to evaluate emotional reactions of customers with respect to given product based on non-verbal self-reporting of 14 emotions which seven of them are positive and others are negative. Positives emotions are: desire, pleasant surprise, inspiration, amusement, admiration, satisfaction, fascination and negatives emotions are: indignation, contempt, disgust, unpleasant surprise, dissatisfaction, disappointment, and boredom. Fourteen emotions is depicted with animated cartoon characters, expressing the emotion through dynamic facial, bodily, and vocal expression. The animated cartoons are made based on the Ekman (1994) who found the facial expressions of basic emotions (fear and joy) which are recognized calculable and obviously across cultures (Desmet, 2005).
2.3.4.1.3 Emo Card
Emo card is a solution to characterize emotions by using pictograms instead of words. Desmet divides the emotions into 8 different categories, and represents each emotion through two facial expressions, of female and male faces. Figure X shows these 16 emocards of the 8 introduced emotional expressions (Desmet, 2011)
2.3.4.1.4 Physiological reaction –ANS (Autonomic Nervous System)
Blood pressure responses, skin responses, brain waves, heart responses, and pupillary responses. EEG, ECG, FMRI, PET helps us to record physiological reactions.
Fear is an emotions with many physical reactions such as increasing heart rates, breathing faster, drier mouth, tense muscles, wet palms which are mediated by controlling heart muscle, smooth muscle, and exocrine glands (Kandel, Schwartz, and Jessell, 2000).Thanks to technology for helping us to recording, measuring and comparing these physical reactions. Researchers in the affective computing field are most active in ANS instruments are IBM’s emotion mouse (Ark, Dryer, & Lu, 1999) Affective Computing Group at MIT designed a range of wearable sensors (e.g. Picard, 2000).
2.3.4.1.4.1 Electromyography (EMG)
EMG helps us to have some data about muscle tensions. High muscle tension happen in stressful situation (Wei, 2013).
2.3.4.1.4.2 Electrodermal Activity
Electrodermal activities are related to Skin Conductivity (SC) or Galvanic Skin Response (GSR). Sweat in palms increase under stressful situations but unfortunately out side temperature can easily interfere on the result, so it needs reference measurements and calibration (Lykken, and Venables, 1971).
2.3.4.1.4.3 Skin Temperature
Measuring skin temperature is easy. Skin temperature decrease in stressful situation, mainly because of the contraction of the blood vessels because of the muscle tension.
2.3.4.1.4.4 Blood Volume Pulse (BVP)
The Blood volume pulse measures the amount of blood currently running though the vessels sited under a photoplethysmograph (PPG) . BVP measures the vasoconstriction of the participant and his/her heartbeat rate which are higher and faster under stress (Kandel, Schwartz, and Jessell, 2000).
2.3.4.1.4.5 Electrocardiogram (ECG)
chest or on the limbs. ECG can be used to measure heart rate (HR) and inter-beat intervals (IBI) to determine the heartbeat rate variability (HRV). A low HRV shows a state of relaxation, whereas an increased HRV shows a potential state of mental stress or frustration (Haag, Goronzy, Schaich, and Williams, 2004).
2.3.4.1.4.6 Respiration Sensor
Respiration sensors measure how deep and fast a person is breathing. Fast and deep breathing shows excitement, anger, fear or joy. Rapid and shallow breathing shows tense Slow and deep breathing shows a relaxed resting state or states of withdrawal, passive like depression or calm happiness.
2.3.4.1.4.7 FMRI
The Functional Magnetic Resonance uses an MRI scanner to measure the blood oxygenation achieving information the amount of stimulation in which part of the brain. The changes amount of oxygenation associated with the underlying synaptic activity. (Ariely, and Berns, 2010; Khalid, and Helander, 2006; Reimann, Zaichkowsky, Neuhaus, Bender, and Weber, 2010 )
2.3.4.1.4.8 PET
Positron Emission Tomography (PET) is a highly specialized imaging technique to know brain functions and body's biological function.
2.3.4.1.4.9 EEG
EEG uses electrodes applied to the scalp and measures changes in the electrical field of the brain region underneath. Jenkins, Brown, and Rutterford (2009). EMG, TMS are other kind of measuring emotions which are working with Magnetic.
2.3.4.1.4.10 Eye Tracking
Eye tracking records eyes movements with a special contact lens, mirror and magnetic field sensor (Robinson, 1963). The measurement of eye movement can happen in horizontal, vertical and torsion directions Duchowski, 2007). Eye tracking has been used on research in Psychology, visual system and cognitive linguistic.
2.3.4.1.4.11 Optimal Tracking
Optical tracking, light reflects from the eyes then recorded by a video camera or a kind of optical sensor. Then the information will be analyzed to extract eye rotation from changes in reflections (Crane, Steele, 1985)
2.3.4.1.4.12 Body Tracking
In body tracking interaction between product and user will be tracked in the body (Slater, and Usoh, 1994). Hand tracking is a part of bodytracking by infrared tracking systems like the Vicon and Elite system (Murradius, Goulermas, and Fernando, 2003; Ferrigno, and Pedotti 1985) or by fluorescent gloves and Kinect cameras (Xia, Chen, and Aggarwal, 2011).Nowadays, i capturing the movement and the posture of users is possible. Yacoob and Davis made a dictionary for converting motions of edge of the mouth, eyes and eyebrows, to a linguistic, frame, mid-level representation (Yacoob, Davis,1994).
2.3.4.2- Verbal Instrument (Subjective)
Nonverbal instruments have some limitation and it leads us to use self reported instruments to know subjective feeling. Verbal instruments are a solution to the problems associated to nonverbal instruments. These instruments can have response for all kind of emotions and have a ability of using