SKULL BASE SURGERYNOLUME 6, NUMBER 2 APRIL 1996
TECHNICAL
NOTE
Fronto-Orbito Zygomatic
Approach:
A
Technical
Modification
Aldo Spallone, M.D., Antonella Rizzo, M.D.,
Alexander N.
Konovalov, M.D.,
and Renato
Giuffre, M.D.
The introduction of the techniques of cranial base
surgeryhasofferedanunquestionable contributiontothe neurosurgical treatment of certain difficult deep-seated
lesions. The practice of skull base surgery demands a
particular skill, which mainly results from longtraining with the modem techniques of bone microdissection. It
alsorequires theavailabilityof modemtechnology such
ashigh-powered drills and oscillating-vibrating saws.
The fronto-orbito zygomatic approach ispartof the
technical armamentariumacranial basesurgeoncan use
fordealing with lesions located in the area ofsuperior
orbitalfissure,cavemoussinus,thepetrousapex,and the interpeduncular fossa. As described in the literature,1'2
this approach requires acomplex instrumentarium tobe
performed,asdoesanycranial basesurgery.We describe
here a technical modification which enables this useful
cranial boneflaptobe raised andreplacedwithoutcostly modem technology.
MATERIALS
AND
METHODS
A curvilinear skin incision isperformed starting 3
cmbelow thezygomatic processinfront of the external auditorymeatusjustbehind the superficial temporal
ar-tery, and terminates 4 cm past the midline behind the
hairline. After the skin flap is reflected anteriorly with fish hooks, the frontal pericranium is elevated ina
posterior-to-anterior direction until the supraorbital nerve is
ex-posed and can be mobilized away from the orbit. The periorbitais then visualized andcarefully dissectedaway
from the orbital wall.Thenthezygomaisfully exposed,
usingatechniquedescribed inaprevious paper3for pre-venting injuryof the frontal branchesof the facialnerve.
Briefly, soft tissue dissection is conducted between the deep layerof thesuperficialtemporalfascia and thedeep temporal fascia,and thezygomaisexposed
subperioste-125
Skull BaseSurgery,Volume6,Number2, April1996 DepartnentofNeurosurgeryUniversityof Rome"TorVergata" (A.S.,R.G.),ClinicsNuova
Latina, Rome, Italy, (A.R.),Institute ofNeurosurgery"N.N.Burdenko"(A.N.K.), Moscow,Russia. Reprintrequests:Dr.AldoSpallone, Dept.of Neurosurgery,UniversityofRome,"TorVergata,"Via 0. Raimondo8,00173 Rome, Italy CopyrightX 1996byThiemeMedicalPublishers, Inc.,
SKULL BASESURGERYNOLUME 6, NUMBER 2 APRIL 1996
DRILL CRANIOTOME RONGEUR GIGLl'S SAW PATHOFGIGLI'S SAW
Figure 1. Graphic
representa-tion of fronto-orbito zygomatic
ap-proach. Path of Gigli's saw is
indi-cated (arrows).
allyuntilafull view of thefronto-orbito zygomaticregion
is obtained. Thetemporalis muscle is detachedfromthe temporalfossa toexpose the lateral orbital wall. At this time, a key burr hole is made below the temporal line
which exposes the orbital content and the basal frontal dura, whicharetobeconnected with asupraorbital
fron-tal burr hole as described by Al-Mefty (Fig. 1).4 Two
additional key burr holes,onein thefronto-temporal and
another in the temporal region, can now be made to
completethecraniotomy,ifacraniotome isnotavailable.
Then the lateral orbital wall isremoved witheitheradrill orwithconventionalrongeurs,and thezygomaticprocess is transected close to the mandibular joint using the Gigli'ssaw. Two small holesare drilledjustbefore
com-pleting the zygomatic resection,tobe usedfor
reapprox-imation at the end of the procedure. The Gigli's saw is
then passedfrom the inferior angle of theproximal por-tion of the zygomatic process in front and below the
zygomaticarch above thetemporalis muscle,inthe direc-tion of theexposed lateral orbital wall. A curved
instru-ment such as a long curved mosquito forceps can be a
useful tool forproperly driving the Gigli's saw into this
limitedspace(Fig. 2). Withanassistantretracting
down-wards the skin flap together with the reflected soft
tis-sues, anobliquecutismade in thezygomatic arch, taking
care todirect theGigli's sawnot too forcefullyto avoid theloosening andsubsequent fracturingofthe arch. The
oblique direction the surgeon is obliged to maintain for
moving theGigli's saw inthisnarrow space would
pre-ventinadvertentopeningof themaxillary sinus. The bone flapcanbeliftedupafter the temporalburr holeand the
"keyhole"areconnected withrongeurs.Exposureofthe
temporalduracanbeamplifiedasrequired bymeansofa
basal temporal craniectomy following elevation of the bone flap and downward deflection of the temporalis muscle(Fig. 3).Inadditiontothoseholesmadeinthe
zy-gomaticprocess, onepairofsmall holes is drilled in the
126 frontal region, sufficient for reapproximating the bone
Figure2. Transectionof thezygomatic arch is shown. Notetheoblique direction of the Gigli's saw.
Figure3. Fronto-temporalduraexposureafter
fronto-orbitozygomatic boneflap elevation. 0
/A
FRONTO-ORBITO ZYGOMATICAPPROACH-SPALLONE ETAL
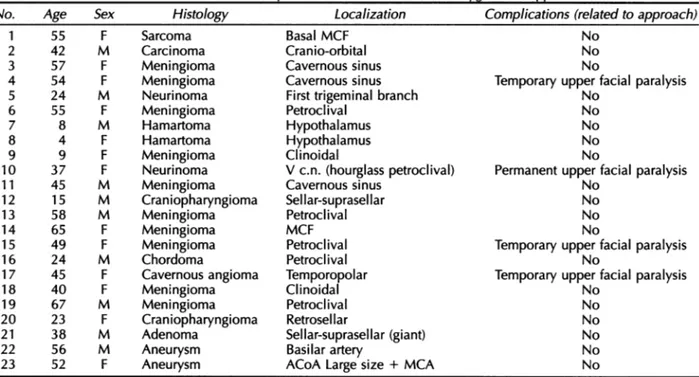
1. SeriesofPatientsOperated onwith Fronto-Orbito-Zygomatic Approach*
Histology Sarcoma Carcinoma Meningioma Meningioma Neurinoma Meningioma Hamartoma Hamartoma Meningioma Neurinoma Meningioma Craniopharyngioma Meningioma Meningioma Meningioma Chordoma Cavernousangioma Meningioma Meningioma Craniopharyngioma Adenoma Aneurysm Aneurysm Localization Basal MCF Cranio-orbital Cavernoussinus Cavernous sinus First trigeminal branch Petroclival Hypothalamus Hypothalamus Clinoidal Vc.n. (hourglass petroclival) Cavernous sinus Sellar-suprasel lar Petroclival MCF Petroclival Petroclival Temporopolar Clinoidal Petroclival Retrosel lar Sellar-suprasellar (giant) Basilarartery
ACoA Large size + MCA
Complications (relatedtoapproach) No
No No
Temporary upperfacial paralysis No
No No No No
Permanentupperfacial paralysis
No No No No
Temporaryupperfacial paralysis
No
Temporary upperfacial paralysis
No No No No No No *Cases1 to 16inMoscow; cases 17 to 23 inRome.
flapusing twosilksutures. In ourexperience, bone flap
healeduneventfully inmore than20 cases-inthe vast
majority,cranial basepathologicalprocesses-inwhich
itwas utilized(Table 1).
Illustrative Case
MRI (Fig.5) showedaright clinoidalmeningioma. The
lesionwasremoved followingconvenientexposureusing a right fronto-orbito zygomatic approach (Fig. 6). The
post operativecourse wasuneventful.
DISCUSSION
A40-year-oldwomanpresentedwitha6-month
his-toryof visual loss in righteye, headache, epileptic sei- Theinterest ofthepresentcommunicationrests on
zures, andbehavioraldisturbances. CT scan(Fig. 4) and thefact thatacomplex bone flap suchastheonedescribed
sf
-
_
Figure 4. CT of a 40-year-old
womanwitha6-monthhistoryof visual
loss in the right eye, headache,
epi-leptic seizures, and behavioral
distur-bances. Rightclinoidal meningioma. 12
No. 1 2 3 4 5 6 7 8 9 10 1 1 12 13 14 15 16 17 18 19 20 21 22 23 Age 55 42 57 54 24 55 8 4 9 37 45 15 58 65 49 24 45 40 67 23 38 56 52 Table Sex F M F F M F M F F F M M M F F M F F M F M M F
SKULL BASE SURGERYNOLUME 6, NUMBER 2 APRIL 1996
Figure
5.Angio-MRI
of thesamepatient gives
further details of the meningioma.
.4IP~~~~~~~~~4
:
Figure
6.Postoperative
control CTdemonstrates total removal of the lesionhere can be elevated and effectively replaced without complextechnology.
Gigli's saw is a time honoredneurosurgical
instru-ment5;however, its use has steadily decreased in the last few years due to theintroduction ofhigh-powered instru-ments. As aresult, young neurosurgeons completing their
trainingindeveloped counties may not be familiarwith thetechniques necessary to master its correct use. Still, theGigli's saw is in auseful instrumentthat may allow neurosurgeons to perform complex cranial bone resec-tions in an environment wherecostly,high-powered,and
complex instrumentsare notavailable. Thus,the advan-tagesof this "low-tech" approachare made available to neurosurgical centers around the world where financial
restraints prevent theacquisition ofcostly,complex tech-nology. This would allow better treatment of cases of basally located lesions such as the one described here,
which do notnecessarily require resectionofthe cranial base, but may benefitfromamorebasallytargeted surgi-cal approach.
Moreover, the use of the Gigli's saw may also de-crease the risk of inadvertent opening of the maxillary
sinus, which ismorethan apurely theoretical risk when anoscillatingsaw is used forcuttingthezygomaticroot,
particularly if the cutting angle is notproperly oriented.
We have used this bone flap technique in over 20 cases, always with an adequate view of thetargeted re-gionand withoutcomplicationsrelated to either elevation orreplacement ofthe boneflap.
REFERENCES
1. Al-Mefty 0:Supraorbital-pterional approachtoskull base lesion. Neurosurgery21:474-477, 1987
2. Brunori A, Bruni P, Greco R,et al: Celebrating the Centennial (1894-1994): LeonardoGigliand hissaw.JNeurosurg 82:1086-1090, 1995
3. IkedaK, Yamashita J, Hashimoto M,etal:Orbitozygomatic tempo-ropolar approach forahighbasilartip aneurysm associated with
ashort intracranial internal carotid artery: A newsurgical ap-proach.Neurosurgery 28:105-110, 1991
4. Hakuba A, LiuS,Nishimura S: Theorbitozygomatic infratemporal
approach:A newsurgical technique. SurgNeurol26:271-276,
1986
5. AmmiratiM,Spallone A,MaJ,etal: Ananatomico-surgicalstudy ofthetemporal branch of the facial nerve. Neurosurgery 33:
1038-1044, 1993