CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports60(2019)327–330ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
j o u r n al ho m e p a g e :w w w . c a s e r e p o r t s . c o m
The
management
of
esophago-gastric
necrosis
due
to
caustics
ingestion:
Anastomotic
reinforcement
with
Cyanoacrylate
glue
and
damage
control
with
Vacuum
Assisted
Closure
Therapy—A
case
report
A.
Picciariello
∗,
V.
Papagni,
G.
Martines,
N.
Palasciano,
D.F.
Altomare
DepartmentofEmergencyandOrganTransplantation,UniversityAldoMoroofBari,Bari,Italy
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14February2019
Receivedinrevisedform16June2019 Accepted19June2019
Availableonline28June2019
Keywords: Gastricnecrosis Cyanoacrylateglue
Esophago-jejunumanastomosis Damagecontrol
Vacuumassistedclosure
a
b
s
t
r
a
c
t
INTRODUCTION:Thesurgicaltreatmentofacompletegastricnecrosisduetocausticingestionisextremely challengingandlifethreatening.Inthisemergencyscenario,afirst-timereconstructionofthe gastroin-testinaltractisoftendangerousforthepatientbecauseofthehighriskofinfectionsandanastomosis leakage.Literaturelacksofclearindicationsforthemanagementofthiscondition.
PRESENTATIONOFCASE:Malepatientwithhistoryofmajordepressiondisorderwasadmittedtoour EmergencyUnitaftertheingestionofmuriaticacid.CTscanshowedmassivepneumo-peritoneumwith esophago-gastricthickening.Freefluidsintheabdominalcavityweredetected.Intraoperativefinding wasacompletenecrosisofthestomachandcorrosionoftheloweresophagus.
DISCUSSION:Inthiscasereportweproposedafirstapproachwiththedrainageandlavageoftheabdomen cavity.Then,anesophago-jejunumanastomosisreinforcedbyCyanoacrylategluewasperformedanda damagecontrolwithVACtherapy(VacuumAssistedClosure)wascarriedout.
CONCLUSION:Cyanoacrylategluecouldbeconsideredusefulandefficientinthereinforcementof anas-tomosiseveninemergencysurgicalprocedures.DamagecontrolusingVACallowstokeepagoodcontrol ofthesurgeryperformed.
©2019TheAuthor(s).PublishedbyElsevierLtdonbehalfofIJSPublishingGroupLtd.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
1. Introduction
Upper gastrointestinal injuries due to caustic ingestion are rare surgical emergencies often associated to intentional sui-cideattemptsinadults[1,2].Theseemergenciesusuallyconcern patientswithanagestartingfrom21yearsold[3].
Thescenarioafteracausticingestionisextremelyvarious, rang-ing froma single perforation of thestomachor an esophageal stricturetoacompletegastricnecrosis[4].
Patientssurvival afterseverecausticgastrointestinalinjuries dependsonthetimeframebetweeningestionandsurgical treat-ment[5].
Esophagogastroduodenoscopyrepresentsthegoldstandardto evaluatetheseverityandtheextensionoftheinjuryanditalso allowstochoosethebesttreatmentforpatients[6].
Itisquitedebatedinliteraturewhatisthebestsurgical proce-duretotreatthiscondition;infactbothonestageandtwostages procedureshavebeenproposed[6,7].
Weaimedtoreportourexperienceinthemanagementof a patientwithseverefull-thicknessgastricwallnecrosisassociated
∗ Correspondingauthor.
E-mailaddress:[email protected](A.Picciariello).
withpartiallowesophagealinjuryaftertheingestionof hydrochlo-ricacid.
Atwo-timesurgerywasperformedusingcyanoacrylategluefor thereinforcementoftheesophaho-jejunalanastomosis. Further-more,wecarriedoutadamagecontrolusingVAC(VacuumAssisted Closure)therapyinordertokeepagoodcontrolofsurgery.
ThiscasereportiswrittenaccordingtoSCAREcriteria[8].
2. Presentationofcase
A 64 years old male was admitted to our Emergency Unit showinganxiety,confusionandagitation,pharyngealburnsand epigastricpain.GCS15.
The anamnesis was collectedby his relatives who reported muriaticacidingestionabout5hbeforeFirstAidadmission. Fur-thermore,thepatienthasbeeninastateofmajordepressionfor10 years.Noothercomorbiditiesorprevioussurgerieswerereported. Patient vital signs were BP 100/55mmHg, HR 125/min, RR 22/min,temperature37◦C,weight95Kg,height180cm.
Atphysicalexamination:tendernessoftheabdomen,positive Blumbergsign,absenceofbowelsounds.
Thehemogasanalysis showeda metabolicacidosis (pH7.14) withaslighthypercalcaemia(1,29mmol/L)andahyperchloremia (118mmol/L).
https://doi.org/10.1016/j.ijscr.2019.06.032
2210-2612/©2019TheAuthor(s).PublishedbyElsevierLtdonbehalfofIJSPublishingGroupLtd.ThisisanopenaccessarticleundertheCCBYlicense(http://creativecommons. org/licenses/by/4.0/).
CASE
REPORT
–
OPEN
ACCESS
328 A.Picciarielloetal./InternationalJournalofSurgeryCaseReports60(2019)327–330Fig.1. SpecimenTotalgastrectomywithomentectomy.
Bloodtestsshowedneutrophilicleukocytosisandanincreaseof C-reactiveprotein(112mg/L),Hb16.7g/dlandHct51%,lacticacid 1.8mmol/L.
AtFirstAidanECGwasperformed(sinustachycardia,117bpm) and thepatient underwent a chest x-ray and an Esophagogas-troduodenoscopy(EGDS)showinganextensivemucosalnecrosis (Zargar3B).
The abdomen CT scan demonstrated a massive pneumo-peritoneumwithesophago-gastricthickening.Free fluidsinthe abdominalcavityaroundthestomachweredetected.
Thepatientunderwentemergencysurgery(ASAIVE)andduring thefirstoperationtheabdomenwasexploredwithevidenceofa largeapertureoftheposterior-lateralgastricwallandtotalgastric necrosiswiththepresenceofingestedmaterial.Consideringthe patients’poorperformancestatus,asfirstapproachthreetubular drainswereputintheabdomenafteralavage;theapertureonthe posteriorwallofthestomachwasclosedandthenecrotictissues wasremoved.Inthesecondoperation(18hafter)atotal gastrec-tomywithomentectomy(Fig.1)andastapledfunctionalside-to sideesophago-jejunal(E-J)anastomosisontheanterioresophageal wallwereperformed.Anendtosidejejuno-jejunalanastomosis wascarriedouttorestorethegastrointestinaltransit.
CyanoacrilategluewasusedtoreinforcetheE-Janastomosisand damagecontrolwithVAC(VacuumAssistedClosure)(Fig.2)was carriedoutinordertokeepagoodcontrolandtoallowasecond looksurgery.
After48hVACSystemwasremovedandtheanastomosiswas checkedwithanesophagojejunoscopywithanairleaktest (neg-ative).TheabdomenwasclosedwithinterruptedVicryl1forthe fascia.
Onpostoperativeday(POD)5thepatientunderwentparenteral nutritionin theIntensiveCareUnitandonPOD8 atemporary tracheostomywasperformedandthepatientstartedtodrink.
OnPOD14hehadapneumoniatreatedbyantibiotictherapyand on22PODhewasmovedtothePsychiatryUnitwherehestarted atherapyforthemajordepressionandasemisoliddiet.
OnPOD26afurtheresophagojejunoscopydemonstratedthe absenceofleakage anda good transitthroughtheanastomosis
Fig.2.VacuumAssistedClosureTherapy.
Fig.3.EndoscopiccontrolonPOD26.
(Fig.3).Thewoundhealingwascompletelynormalandthepatient wasdischargedonPOD33.
3. Discussion
MassiveIngestionofcorrosivesubstancesforsuicidalintentin adultsrepresentsasurgicalemergencywithahighrateofmortality (about20%)andlong-termconsequences[9].Therealprevalence oftheseinjuriesisunderratedbecauseliteraturelacksofreviews andincludesonlyrandompapersandcasereports/caseseries.
InjuriesfromcausticsubstancesaremorecommoninWestern countriesthanindevelopingcountrieswherepeoplecaneasilyfind acidswhichareusedforsuicidalintent[10].
Lesionsaftercausticingestionaremoreseverinadults,maybe duetothemassiveamountofcausticingested[1].Among devastat-ingconsequencesduetocausticingestion,severeinjuries,suchas necrosisoftheoesophagusand/orthestomach,canoccurleading toshortandlongtermlife-threateningcomplications[11].
Mostoftimes,thefirstapproachisalife-savingmedical ther-apyperformedtokeepthepatientstable(e.vfluids,antibioticsand electrolytescorrection)and,ifnecessary,anorotrachealintubation toassessairwaysafety[9].
Eveniftherearenostrictguidelinesregardingtheindication ofendoscopyaftertheingestionofalargeamountofcorrosives,
CASE
REPORT
–
OPEN
ACCESS
A.Picciarielloetal./InternationalJournalofSurgeryCaseReports60(2019)327–330 329
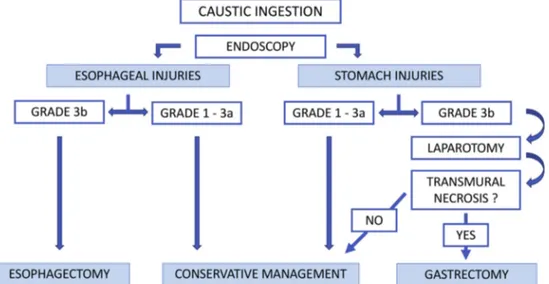
Fig.4.Algorithmforemergencymanagementofcausticinjuries.
Table1
Zargar’sgradingclassificationofmucosalinjurycausedbyingestionofcaustic substances.
GRADE DESCRIPTION
0 Normalexamination
1 Edemaandhyperemiaofthemucosa
2a Superficialulceration,erosions,friability,blisters, exudates,hemorrhages,whitishmembranes 2b Grade2◦+deepdiscreteofcircumferentialulceration 3a Smallscatteredareasofmultipleulcerationandareasof
necrosiswithbrown/blackorgreyishdiscoloration
3b Extensivenecrosis
4 Perforation
anEGDS,inabsenceofathirddegreeburnofthehypopharynx,is usefultostagetheinjuryandtomakethebestchoicetotreatit [6].Grade3Binjury,accordingtoZargarendoscopicclassification
(Table1),isalife-threateningconditionandanimmediate
laparo-tomyismandatory[11](Fig.4).
AccordingtoCattanetal.thesurgicaltreatmentofseverecaustic injuriesshouldperformedassoonaspossibleinordertoimprove theprognosisofpatients[12].
Data from literature showthe lack of a standardized surgi-calprocedurefornecrosisofstomachand/oroesophagusdueto causticsingestion.Someauthorsreportgoodshortandlongterm outcomesof one-timesurgical treatmentwith esophagojejunal reconstructionaftertotalgastrectomy[11,13].
Ontheotherhand,damagecontrolsurgery(DCS)[14]withthe useofVACsystemcouldbeavalidapproachforlife-threatening conditions. In fact, DCS involves more steps for the treatment and,usually,themainsurgicalprocedureisperformedonlywhen patientsarestable.Inthisway,therateofadversecomplications aftersurgerycouldbelower.
In this case we report our experience using a three steps approach for complete stomach necrosisdue to acidingestion. Firstly,adrainageoftheabdomencavitywasperformed clean-ingtheabdomenbythenecrotictissueandclosingtheaperture ontheposteriorwallofthestomachwitharunningsuture.During thesecondoperationatotalgastrectomyandesophago-jejunum anastomosis reinforced by Cyanoacrylate glue was carried out. Cyanoacrylateglueisasyntheticgluewithsealing,adhesiveand hemostaticpropertieswidelyusedinelectivesurgery[15].Afterthe operation,thepatientunderwentdamagecontrolwithVAC ther-apythatallowedustochecktheconditionoftheanastomosisafter 48h.
VACcouldbeconsideredveryhelpfulforcriticalpatientssince itallowsafasterabdominalclosureandanearlierdischargefrom theIntensivecareUnit[16,17].
4. Conclusion
Ingestionofcausticsubstanceshasdevastatingconsequences ontheesophagusandthestomachandoftenemergencysurgery is required. Cyanoacrylate glue couldbe considereduseful and efficientinthereinforcementofanastomosiseveninemergency surgicalprocedures.DamagecontrolusingVACallowstohavea goodcontrolofthesurgeryperformedandtomakearevisionofthe abdomentwodaysafterthecriticalsurgicalprocedureandbefore theclosureoftheabdomen.
Conflictsofinterest
Noconflictofinteresttodeclaire.
Funding
Nofoundingreceived.
Ethicalapproval
EthicalapprovalwasobtainedbyInternationalReviewBoard ofAziendaOspedalieraUniveristaria–PoliclinicodiBari,P.zzaG. Cesare,Bari,Italy
Consent
Writteninformedconsentwasobtainedfromthepatientfor publicationofthiscasereportandaccompanyingimages.Acopy ofthewrittenconsentisavailableforreviewbytheEditor-in-Chief ofthisjournalonrequest.
Authorcontribution
Arcangelo Picciariello: conception of studydesign, data col-lection, analysis, manuscript writing, revision and manuscript submission.
PapagniVincenzo:conceptionofstudydesign,datacollection, analysis,revisionofthemanuscript.
CASE
REPORT
–
OPEN
ACCESS
330 A.Picciarielloetal./InternationalJournalofSurgeryCaseReports60(2019)327–330GennaroMartines:criticalrevisionofthemanuscript,approved thefinalversionofthemanuscriptforsubmission.
NicolaPalasciano:datacollection,analysis,manuscriptwriting andrevision.
DonatoF.Altomare:manuscriptwriting,drafting,revisingofthe manuscriptandparticipationinthecareofthepatient.
Registrationofresearchstudies
Thisstudydoesnotrequiretheregistration.
Guarantor
ArcangeloPicciariello,MD.
Provenanceandpeerreview
Notcommissioned,externallypeer-reviewed.
References
[1]A.I.Vezakis,etal.,Clinicalspectrumandmanagementofcausticingestion:a caseseriespresentingthreeopposingoutcomes,Am.J.CaseRep.17(2016) 340–346.
[2]J.B.Mowry,etal.,2014AnnualreportoftheAmericanAssociationofPoison ControlCenters’NationalPoisonDataSystem(NPDS):32ndAnnualreport, Clin.Toxicol.(Phila)53(10)(2015)962–1147.
[3]S.B.Schaffer,A.F.Hebert,Causticingestion,J.StateMed.Soc.152(12)(2000) 590–596.
[4]M.Lupa,etal.,Updateonthediagnosisandtreatmentofcausticingestion, OchsnerJ.9(2)(2009)54–59.
[5]E.Sarfati,etal.,Tracheobronchialnecrosisaftercausticingestion,J.Thorac. Cardiovasc.Surg.103(3)(1992)412–413.
[6]H.T.Cheng,etal.,Causticingestioninadults:theroleofendoscopic classificationinpredictingoutcome,BMCGastroenterol.8(2008)31. [7]D.Gossot,E.Sarfati,M.Celerier,Immediateoesojejunalanastomosisafter
totalgastrectomyincausticnecrosis,Ann.Chir.43(5)(1989)352–355. [8]R.A.Agha,etal.,TheSCARE2018statement:updatingconsensusSurgical
CAseREport(SCARE)guidelines,Int.J.Surg.60(2018)132–136.
[9]S.Contini,C.Scarpignato,Causticinjuryoftheuppergastrointestinaltract:a comprehensivereview,WorldJ.Gastroenterol.19(25)(2013)3918–3930. [10]S.A.Zargar,etal.,Ingestionofcorrosiveacids.Spectrumofinjurytoupper gastrointestinaltractandnaturalhistory,Gastroenterology97(3)(1989) 702–707.
[11]M.Chirica,etal.,Esophagojejunostomyaftertotalgastrectomyforcaustic injuries,Dis.Esophagus27(2)(2014)122–127.
[12]P.Cattan,etal.,Extensiveabdominalsurgeryaftercausticingestion,Ann. Surg.231(4)(2000)519–523.
[13]F.Ismael,etal.,Immediateesophagojejunalanastomosisaftertotal gastrectomyforcausticnecrosis.Aproposof5cases,J.Chir.(Paris)133(3) (1996)132–133.
[14]R.Cirocchi,etal.,Damagecontrolsurgeryforabdominaltrauma,Cochrane DatabaseSyst.Rev.(3)(2013)CD007438.
[15]G.M.Bot,etal.,Theuseofcyanoacrylateinsurgicalanastomosis:an alternativetomicrosurgery,J.Surg.Tech.CaseRep.2(1)(2010)44–48. [16]R.Cirocchi,etal.,Whatistheeffectivenessofthenegativepressurewound
therapy(NPWT)inpatientstreatedwithopenabdomentechnique?A systematicreviewandmeta-analysis,J.TraumaAcuteCareSurg.81(3)(2016) 575–584.
[17]S.Batacchi,etal.,Vacuum-assistedclosuredeviceenhancesrecoveryof criticallyillpatientsfollowingemergencysurgicalprocedures,Crit.Care13 (6)(2009)R194.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.