Pleasecitethisarticleinpressas:MarchiS,etal.SeroprevalencestudyofToscanavirusandvirusesbelongingtotheSandflyfever NaplesantigeniccomplexincentralandsouthernItaly.JInfectPublicHealth(2017),http://dx.doi.org/10.1016/j.jiph.2017.02.001
ARTICLE IN PRESS
G Model
JIPH-707; No.ofPages4
JournalofInfectionandPublicHealthxxx(2017)xxx–xxx
Contents lists available atScienceDirect
Journal
of
Infection
and
Public
Health
j o u r n a l h o m e p a g e :h t t p : / / w w w . e l s e v i e r . c o m / l o c a t e / j i p h
Seroprevalence
study
of
Toscana
virus
and
viruses
belonging
to
the
Sandfly
fever
Naples
antigenic
complex
in
central
and
southern
Italy
Serena
Marchi
a,
Claudia
M.
Trombetta
a,
Otfried
Kistner
b,c,
Emanuele
Montomoli
a,c,∗aDepartmentofMolecularandDevelopmentalMedicine,UniversityofSiena,53100Siena,Italy bIndependentConsultant,Vienna1221,Austria
cVisMederiSrl,EnterpriseofServiceinLifeSciences,53100Siena,Italy
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1September2016
Receivedinrevisedform31January2017 Accepted5February2017 Keywords: Toscanavirus Sandfly Seroprevalence Phlebovirus Italy
a
b
s
t
r
a
c
t
Sandflyfevervirusesaretransmittedbythebiteofphlebotominesandflies;serotypessandflyfeverNaples virus,sandflyfeverSicilianvirusandsandflyfeverCyprusviruscausefebrileillness,whereasToscanavirus (TOSV)maycauseneuroinvasiveinfections.AlthoughTOSVisanimportantcauseofasepticmeningitis incentralandsouthernItaly,inmanycasestheinfectionisasymptomatic,leadingtounderestimationof theactualspreadofthevirus.ThisserosurveyaimedtoassesstheseroprevalenceofTOSVinarandom populationinSiena(Tuscany,centralItaly)in2003–2004and2013–2014andBari(Apulia,southern Italy)in2004and2015.2132serumsamplesweretestedforthepresenceofanti-TOSV/SFNVIgGby meansofELISAandIFAcommercialtests.Seroprevalencerateswerecomparedinthetwocitiesandover aten-yearperiodinthesamecity.SeroprevalenceresultsintheSienapopulation(22.95%in2003–2004 vs26.75%in2013–2014)confirmedtheendemiccirculationofTOSVandcloselyrelatedvirusesincentral Italy,withoutmajorchangesoverthelastdecade,whilenosignificantprevalencewasobservedinBari (2.90%in2004vs1.85%in2015).
©2017TheAuthors.PublishedbyElsevierLimited.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Sandflyfeverviruses(Bunyaviridaefamily,genusPhlebovirus) are widelydistributed in theMediterranean basin, where they are transmitted by thebite of infected phlebotomine sandflies belongingtothegenusPhlebotomus[1].Thefourmostcommon serotypesassociatedwithhumaninfectionsincludesandflyfever Naplesvirus(SFNV),sandflyfeverSicilianvirus(SFSV),sandflyfever Cyprusvirus(SFCV)andToscanavirus(TOSV)[2,3].Clinical dis-ease,knownas“pappatacifever”,usuallypresentsasaself-limiting febrileillness,characterizedbyfever,myalgiaandheadache.TOSV istheonlyserotypeassociatedwithneuroinvasiveinfections;in endemicregions,itisamongthemajorcausesofasepticmeningitis andmeningoencephalitisduringthesummerseason[4–6].
InItaly,themainvectorsofTOSVarethesandflies Phleboto-musperfiliewiandPhlebotomusperniciosus,whicharefoundmainly incentralandsouthernregions.OneserosurveyfoundthatSFNV and SFSVinfectionshad disappearedfrom areaswhere malaria eradicationcampaignshadbeenimplemented[5,6];incontrast,
∗ Corresponding author at: Department of Molecular and Developmental Medicine,UniversityofSiena,53100Siena,Italy.
E-mailaddress:[email protected](E.Montomoli).
neurologicaldiseaseduetoTOSVcontinuedtobeobserved annu-ally[7–12],suggestingthepossibilityofananimalreservoirforthis virus[5].Serologicalsurveyshaveshownthepresenceofanti-TOSV antibodiesinovinesandhorses[13];however,therearenoreliable dataindicatinghumansorothervertebratesasanaturalreservoir [5].
Afterreportsofinfectionintouristsfromnorth-centralEurope andtheUSA[14,15],severalstudieswereconductedonthe cir-culationof TOSVin theareaof Siena (Tuscany);most of these includedpopulationsofsubjectshospitalizedforneurological dis-orders[10,12].
Furtherserologicalanalyseswereperformedonpopulations liv-inginthesamehighlyendemicarea.Thefirstofthese,conducted onasymptomatichouseholdcontactsof centralnervoussystem (CNS)infectionpatients,revealedanti-ToscanavirusIgG seropos-itivityin22%ofsubjectsandIgM/IgGin6%[16].Aseroprevalence studyonapopulationofoccupationallyexposedsubjectsfromthe provincesofSiena,FlorenceandArezzorevealedpositiveanti-TOSV IgGin22.7%intheurbancontrolpopulation[17].These investi-gationsconfirmedthewidecirculation ofTOSVinSienaandits provinceandassociatedthiscirculationbothtoasymptomaticand symptomaticinfectionswithoutCNSinvolvementandtoaseptic meningitisandmeningoencephalitisduringthesummermonths. Arecentretrospectivestudyontheantibodyprevalenceratesof http://dx.doi.org/10.1016/j.jiph.2017.02.001
1876-0341/©2017TheAuthors.PublishedbyElsevierLimited.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Pleasecitethisarticleinpressas:MarchiS,etal.SeroprevalencestudyofToscanavirusandvirusesbelongingtotheSandflyfever NaplesantigeniccomplexincentralandsouthernItaly.JInfectPublicHealth(2017),http://dx.doi.org/10.1016/j.jiph.2017.02.001
ARTICLE IN PRESS
G Model
JIPH-707; No.ofPages4
2 S.Marchietal./JournalofInfectionandPublicHealthxxx(2017)xxx–xxx TOSVamongpatientsresidentinTuscanyandhospitalizedfor
rea-sonsotherthanneurologicalinfections,foundseroprevalencerates of19.8%inadultsand5.8%inchildren,indicatinganage-dependent increaseinTOSV-specificimmunity[18].
OthercasesofTOSVinfectionand highseroprevalencerates havebeenreportedinsouthernItalian regions,suchas Campa-nia[19]andSicily[20,21],thusexpandingthegeographicalarea ofcentralItalydefinedinthefirststudies.
Theprimarypurposeofthepresentsurveywastobetter char-acterizethedistributionofTOSVinfectionintheterritoryofSiena overthelastdecade.Thesecondaimwastoinvestigatethe circu-lationofthevirusintheprovinceofBari(Apulia,SouthernItaly).In thislatterarea,epidemiologicaldataonTOSVarelacking,but cir-culationofthevirusissuggestedbypreviousstudiescarriedoutin otherregionsofsouthernItaly.Comparingtheseroprevalencerates inSienaandBariprovidesafullerdescriptionoftheepidemiology ofTOSVintwodifferentItalianregions.
Materialsandmethods
Testswereperformedonhumanserumsamplesfromthe inter-nal serum bank of the Laboratory of Molecular Epidemiology, DepartmentofMolecularandDevelopmentalMedicine,University ofSiena.Thesampleshadbeenanonymouslycollectedin compli-ancewithItalianethicslaw;theonlyinformationavailableonthese subjectswasageandgender.
Atotalof2132serumsamplesfromsubjectsofbothsexesandall ages,collectedinSienainthetwo-yearperiods2003–2004(n=903) and2013–2014(n=836)andinBariin2004(n=333)and2015 (n=60),weretestedforthepresenceofspecificanti-TOSV/SFNV IgGantibodies.
SerologicaltestswereperformedbymeansofEnzywellToscana virusIgG(DIESSE-Siena,Italy)commercialkitbasedonaprinciple ofenzyme-linkedimmunosorbentassay(ELISA)withrecombinant nucleoprotein[22],inaccordancewiththemanufacturer’s instruc-tions. Accordingto themanufacturer, thetest has a sensitivity of95%andspecificityof96.5%;furthermore,cross-reactionswith othercorrelatedserotypesofthePhlebovirusgenus,suchasSFSV andSFNV,cannotbeexcluded[22].
SerumsampleswithborderlineELISAresults(accordingtothe parametersoftheELISAkit)wereexcludedfromthestudy,while thosewithpositiveresultsunderwentconfirmatory immunoflu-orescenceassay (IFA)by meansof the commercialkit “Mosaic Sandflyfevervirus1”(Euroimmun,Germany)asindicatedbythe manufacturer.The IFA distinguishesIgGfor thefourserotypes: SFSV,SFNV,SFCVandTOSV.Consideringthatitisimpossiblewith ELISAandIFAteststodistinguishbetweenTOSVIgGandIgGraised after infection caused by another virus belonging to the same antigeniccomplex,samplespositive toTOSVIgGareconsidered positiveforTOSV/SFNVIgG[1].
Sex- and age-specific seroprevalence rates were calculated, alongwiththecorresponding95%confidenceintervals(CI). Sta-tisticalanalysiswasperformedbymeansoftheYatescorrected chi-squaretesttocompareprevalenceratesamongdifferentstudy groups.StatisticalsignificancewassetatP<0.05,two-tailed.
Results
Atotalof2132serumsamplesweretestedbyELISAassay,125 ofwhich yieldedborderlineresultsand2 werenotsuitable for IFA.These127sampleswereexcludedfromthestudy,while691 sampleswithELISApositiveresultsweretestedbyIFA.
SampleswithIFA negativeresultsfor TOSVwereconsidered negativealongwiththosewithELISAnegativeresults.Only
sam-Table1
Seroprevalenceofanti-TOSV/SFNVIgGbyIFAinSienapopulation2003–2004and 2013–2014,dividedbyage-group.
Agegroups Siena,2003–2004(%) Siena,2013–2014(%)
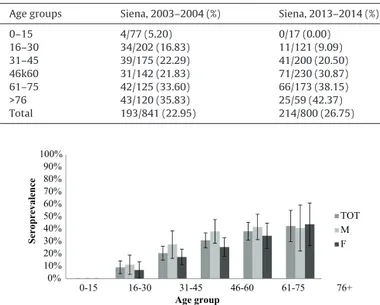
0–15 4/77(5.20) 0/17(0.00) 16–30 34/202(16.83) 11/121(9.09) 31–45 39/175(22.29) 41/200(20.50) 46k60 31/142(21.83) 71/230(30.87) 61–75 42/125(33.60) 66/173(38.15) >76 43/120(35.83) 25/59(42.37) Total 193/841(22.95) 214/800(26.75) 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 0-15 16-30 31-45 46-60 61-75 76+ Sero preva le nc e Age group TOT M F
Fig.1. Prevalenceofanti-TOSV/SFNVIgGbyIFAinSienapopulationin2013–2014, byage-groupandsex,with95%CI.
Table2
Prevalenceofanti-TOSV/SFNVIgGbyIFAinpopulationofBari2004and2015, dividedbyage-groups.
Agegroups Bari,2004(%) Bari,2015(%)
0–15 0/32(0.00) 0/6(0.00) 16–30 0/77(0.00) 1/12(8.33) 31–45 0/71(0.00) 0/13(0.00) 46–60 1/54(1.85) 0/9(0.00) 61–75 5/55(9.09) 0/8(0.00) >76 3/21(14.29) 0/6(0.00) Total 9/310(2.90) 1/54(1.85)
pleswithTOSVIFApositiveresultswereconsideredtobepositive
foranti-TOSV/SFNVIgG.
Samplesweredividedby genderand classifiedintosix
age-groups:0–15,16–30,31–45,46–60,61–75and>76yearsold.
Theresultsforanti-TOSV/SFNVIgGinsamplescollectedinSiena
in2003–2004and 2013–2014are reportedinTable1; 193/841
(22.95%,CI:20.11–25.79)samplescollectedinSienain2003–2004 werepositive for anti-TOSV/SFNVIgG (Table1), whilesamples collectedinthesameareain2013–2014dispilayedTOSV/SFNV seropositivityof26.75%(214/800,CI:23.68–29.82)(Table1).No significantdifferenceinTOSV/SFNVseroprevalencewasobserved betweenthetwo-yearperiodsconsidered(P=0.085).
On considering the biennium 2013–2014, TOSV/SFNV sero-prevalencewassignificantlylower(P=0.011)infemales(23.11% CI:19.22–27.01)thaninmales(31.43%CI:26.56–36.29).On sub-dividing the age-groups by sex, the prevalence rate found in samplesof46–60yearsoldmales(38%,CI:28.49–47.51)collected in2013–2014wassignificantlyhigherthanthatofthesame age-groupinthe2003–2004population(20%,CI:9.88–30.12)(P=0.028) (Fig.1).
Moreover,theprevalenceofanti-TOSV/SFNVIgGsignificantly increased(P<0.001)withage.Indeed,seroprevalencedisplayeda linearage-relatedincrease:from0%inchildren<15years oldto 42.37%(CI:29.76–54.98)intheelderly(Fig.1).Noothersignificant differences,bysexoryearofcollection,wereobserved.
TOSV/SFNVseroprevalenceinsamplescollectedinBariin2004 and2015arereportedinTable2.Of310samplescollectedinBariin 2004,only9werepositiveforTOSV/SFNVIgG(2.90%,CI:1.03–4.77) (Table2).Asmallnumberofsamplescollectedinthesamearea
Pleasecitethisarticleinpressas:MarchiS,etal.SeroprevalencestudyofToscanavirusandvirusesbelongingtotheSandflyfever NaplesantigeniccomplexincentralandsouthernItaly.JInfectPublicHealth(2017),http://dx.doi.org/10.1016/j.jiph.2017.02.001
ARTICLE IN PRESS
G Model
JIPH-707; No.ofPages4
S.Marchietal./JournalofInfectionandPublicHealthxxx(2017)xxx–xxx 3 Table3
Prevalenceofanti-TOSV/SFNVIgGbyIFAinpopulationof2004inBariandinSiena dividedbyage-groups.
Agegroups Bari,2004(%) Siena,2004(%)
0–15 0/32(0.00) 3/37(8.11) 16–30 0/77(0.00) 14/82(17.07) 31–45 0/71(0.00) 11/58(18.97) 46–60 1/54(1.85) 15/69(21.74) 61–75 5/55(9.09) 20/76(26.32) >76 3/21(14.29) 27/79(34.18) Total 9/310(2.90) 90/401(22.44) 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 0-15 16-30 31-45 46-60 61-75 76+ Seroprevale nce Age group BARI SIENA
Fig.2. Prevalenceofanti-TOSV/SFNVIgGbyIFAinSienaandBariin2004,by age-group,with95%CI.
Table4
SamplestestedbyIFAwithpositiveresultsforSFSVSFNVandSFCVinSienain 2003–2004and2013–2014andinBariin2004and2015.
Agegroups Siena 2003–2004 (%) Siena 2013–2014 (%) Bari2004 (%) Bari2015 (%) SFSV 0/299(0.00) 6/332(1.81) 4/60(6.67) 0/1(0.00) SFNV 8/299(2.68) 1/332(0.30) 4/60(6.67) 0/1(0.00) SFCV 1/299(0.33) 2/332(0.60) 0/60(0.00) 0/1(0.00)
in 2015weretested; 1/54(1.85%) showed anti-TOSV/SFNVIgG
(Table2).Noothersampleswereavailablefortesting;nosignificant differencewasfoundbetweenthetwoyears(P=1.00).
TheresultsobtainedfromsamplesfromBariin2004(n=310) werecomparedwiththoseofsamplescollectedinSienainthesame year(n=401)(Table3,Fig.2).ThedifferencebetweenTOSV/SFNV seroprevalence rates was highly significant(P<0.001). Regard-ingthedistributionamongage-groups,nodifferencewasfound betweenchildrenaged0–15yearsinbothcities,whileavery sig-nificantdifferencewasfoundinadults,especially inthoseaged 16–30and31–45years(P<0.001).
Of691samplestestedbyIFA,26sampleswerenegativefor anti-TOSV/SFNVIgG butshowedpositivitytooneoftheotherthree serotypesthatcouldberecognizedwithIFA(Table4).
Discussion
TOSVisanarbovirustransmittedbysandfliesofthegenus Phle-botomus,whicharewidespreadincentralandsouthern Italy.In manycases,theinfectionisasymptomaticorassociatedwith flu-likesymptoms,resultinginunderestimationoftheactualspreadof thevirus.Nevertheless,inendemicareas,TOSVisamongthemajor causesofasepticmeningitisandmeningoencephalitisduringthe summerseason.InItaly,thevirusismainlyfoundinthecentral regions,butithasalsobeenobservedinthesouth[5,6].
Thisserologicalsurveywasconductedinordertoestimatethe prevalenceofanti-TOSVantibodiesinthegeneralpopulationsof Siena(CentralItaly)andBari(SouthernItaly)overthelastdecade,
andtomakeacomparisonbetweenthesetwodifferent geograph-icalareas.
Analysisof thedata obtainedfromthis survey confirms the resultsreportedbypreviousstudies[10,12,16,17].Inparticular,the resultsfromtheSienapopulationin2003–2004areconsistentwith thosereportedinaserologicalsurveyconductedinapopulation liv-inginTuscanyduringtheperiodof1999–2006[18],whichshowed aTOSVseroprevalenceof5.8%inchildrenand19.8%inadults.The TOSV/SFNVseroprevalenceobservedin2003–2004(22.95%)andin 2013–2014(26.75%)confirmsSienaasanendemicareaandthatno significantchangeshaveoccurredoverthedecade.
In the2013–2014studypopulationinSiena,31.43% ofmale and 23.11% of female subjects showed TOSV/SFNV immunity (P=0.011).Moreover,theprevalencerate(38%)foundinmale sub-jectsagedfrom46to60yearswassignificantlyhigherthanthat reportedfor46–60yearoldmalesin2003–2004(P=0.022). Unfor-tunately,asspecimenswerenotaccompaniedbyananamnestic questionnaire,itwasnotpossibletoassociateTOSV/SFNV seropos-itivitywithfactorsthatmayincreasetheriskofinfectioninthe subgroupconsidered.However,itcanbeassumedthatsome out-dooractivitiesrelatedtoagreaterriskofinfection,suchasforestry andfarming[23],aremorefrequentlypracticedbysome popula-tionsubgroups.
TheTOSV/SFNVseroprevalenceobservedalongage-groupswas significantlylowerinchildren(P=0.001)andshowedalinear age-related increase. Less exposuretothe vectorcould explain the virtualabsenceofTOSV/SFNVspecificimmunityinsubjectsless than 15years old. Considering only subjects over 15years old, inSienain2013–2014TOSV/SFNVseroprevalenceobservedwas 27.33%(23.53%in femalesand32.26%in males),indicatingthat theinfectionis morefrequentinadults.Specifically,insubjects aged61–75andover76years,thepercentageofpositivityreached 38.15%and42.37%,respectively.Confirmingtheresultsofprevious epidemiological studies[18],theincreasing seroprevalencerate concurrentwithagedemonstratesthatthepopulationis consis-tentlyexposedtoTOSVorcloselyrelatedvirusesthroughoutlife. Indeed,typicalhillside settlementsin theprovinceofSienaare exposedtogreatercontactwithsandflies,andthereforetoagreater riskofinfectioninallage-groups,assuggestedbyBraitoetal.[23]. StudiesconductedinsouthernItalyhaveindicatedTOSVasthe causeof 5.6%ofmeningitis casesin thesummertimein Naples (Campania)[19]andofhighseroprevalenceratesinSicily[20,21]. Incontrast,samplescollectedintheprovinceofBarididnotshow asignificantprevalenceofTOSV/SFNV,whichwas2.90%in2004 and1.85%in2015.Asnootherepidemiologicalstudieshavebeen conductedintheApuliaregion,itcanbeclaimedthatthisisthe firstsurveyofthepresenceofTOSVandcloselyrelatedvirusesin thisarea.
Moreover,theresultsobtainedfromsamplesfromBariinthe year2004werecomparedwiththoseofsamplescollectedinSiena in thesameyear.The differencebetweentheTOSV/SFNV sero-prevalencerates foundinSienaand Bariwashighly significant (P<0.001).Thismaybeduetothedifferentbiologicalandclimatic nichesofthesegeographicalareas,whichcouldbedifferentially hospitabletothevector.Interestingly,almostallthesamples pos-itivetoanti-TOSV/SFNVIgGthatwerecollectedin theprovince ofBariwerefromsubjectsover61yearsold(8/10),suggestinga greatercirculationofthevirusesinpreviousdecades.
Inthisstudy,reactivitytootherserotypesrecognizablebyIFA was detected in 26 samples in total, 24 of them belonged to over-65-year-oldsubjects.EspeciallyforSFSVandSFNV,these find-ingsareconsistentwithpreviousserologicalstudiesthatobserved thedecreaseordisappearanceoftheseviralinfectionsafterthe 1940smalariaeradicationcampaignsinItaly[8].Apossible cross-reactivitybetweenotherviralserotypesbelongingtothesandfly feverNaplesspeciescannotbefullyexcludedwithouttesting
pos-Pleasecitethisarticleinpressas:MarchiS,etal.SeroprevalencestudyofToscanavirusandvirusesbelongingtotheSandflyfever NaplesantigeniccomplexincentralandsouthernItaly.JInfectPublicHealth(2017),http://dx.doi.org/10.1016/j.jiph.2017.02.001
ARTICLE IN PRESS
G Model
JIPH-707; No.ofPages4
4 S.Marchietal./JournalofInfectionandPublicHealthxxx(2017)xxx–xxx itivesamplesalsobyvirusneutralization[24,25]buttakeninto
accountthegeographicalareaofinterestandtheresultsof pre-viousseroprevalencestudies[8,16–18]seropositiveresultsinthis studyclearlysupporttheclassificationasTOSV-positive.
Themainimportanceofthisstudyisthatthedetectionof anti-TOSV/SFNVantibodieswasconductedonsamplesthathadbeen collectedforother medicalpurposes, not necessarilyrelated to TOSVinfection.Indeed,randomlychoosing a populationallows characterizingthespread oftheviruseven amongmembers of thegeneralpopulationofan endemicarea. On theotherhand, thelackofinformation(e.g.employment,outdooractivities, extra-urbanresidence,petownership,neurologicaldisease,andprevious diagnosis of TOSV infection) on the subjects involved did not allowevaluatingtheinfluenceoffactorsthatmayberelatedtoan increasedriskofinfection.ThisstudyshowsthatinTuscanyisstill anendemicarea,andthatnosignificantchangeinprevalencerates hasoccurredinthelastdecade.InApulia,bycontrast,theviruses seemtobesomewhatrare.
Inconclusion,forresidentsinendemicareas,theprobabilityof beinginfectedbyTOSVandcloselyrelatedvirusesanddeveloping specificantibodiesincreasesduringtheirlifetime.Moreover,CNS infectionsappeartobemorefrequentinadultsthaninchildren [18];therefore,highseroprevalenceamongolderadultsisa con-cern.On theotherhand,populationsinendemicareascouldbe betterprotectedfromneurologicalinfections,owingtorepeated exposuretothevirus, which canboost immunity [26]. Indeed, pathogenicityseemstobehigherinsubjectswhocomefrom non-endemicareas[27];thismaybebecausetheyaremoresusceptible toinfectioninlaterlifeastheydonothavepreviouslyacquired immunityagainstTOSV.Thus,itisnecessarytocontinue monitor-ingthespreadofTOSVinendemicareas,inordertoassesstherisk forthehealthofbothresidentsandtourist.
Funding Nofundingsources. Competinginterests Nonedeclared. Ethicalapproval Notrequired. References
[1]AlkanC,BichaudL,deLamballerieX,AltenB,GouldEA,CharrelRN. Sandfly-bornephlebovirusesofEurasiaandAfrica:epidemiology,geneticdiversity, geographicrange,controlmeasures.AntiviralRes2013;100(1):54–74. [2]PapaA,KonstantinouG,PavlidouV,AntoniadisA.Sandflyfevervirusoutbreak
inCyprus.ClinMicrobiolInfect2006;12(2):192–4.
[3]ShiralyR,KhosraviA,FarahangizS.Seroprevalenceofsandflyfevervirus infec-tioninmilitarypersonnelonthewesternborderofIran.JInfectPublicHealth 2016.
[4]DepaquitJ,GrandadamM,FouqueF,AndryPE,PeyrefitteC.Arthropod-borne virusestransmitted byPhlebotominesandflies inEurope:a review.Euro Surveill2010;15(10):19507.
[5]ValassinaM,CusiMG,ValensinPE.AMediterraneanarbovirus:theToscana virus.JNeurovirol2003;9(6):577–83.
[6]CusiMG,SavelliniGG,ZanelliG.Toscanavirusepidemiology:fromItalyto beyond.OpenVirolJ2010;4:22–8.
[7]NicolettiL,VeraniP,CaciolliS,CiufoliniMG,RenziA,BartolozziD,etal. Cen-tralnervoussysteminvolvementduringinfectionbyPhlebovirustoscanaof residentsinnaturalfociincentralItaly(1977-1988).AmJTropMedHyg 1991;45(4):429–34.
[8]NicolettiL,CiufoliniMG,VeraniP.SandflyfevervirusesinItaly.ArchVirolSuppl 1996;11:41–7.
[9]VeraniP,NicolettiL,CiufoliniMG,BalducciM.Virusestransmittedbysandflies inItaly.Parassitologia1991;33Suppl:513–8.
[10]BraitoA,Ciufolini MG,Pippi L, CorbisieroR,FiorentiniC, GistriA, etal. Phlebotomus-transmittedtoscanavirusinfectionsofthecentralnervous sys-tem:aseven-yearexperienceinTuscany.ScandJInfectDis1998;30(5):505–8. [11]ValassinaM,CupponeAM,BianchiS,SantiniL,CusiMG.EvidenceofToscana virusvariantscirculatinginTuscany:Italy,duringthesummersof1995to1997. JClinMicrobiol1998;36(7):2103–4.
[12]Valassina M,Meacci F, Valensin PE, Cusi MG. Detection of neurotropic virusescirculatinginTuscany:theincisiveroleofToscanavirus.JMedVirol 2000;60(1):86–90.
[13]CilunaMT,ScaramozzinoP,CocumelliC,CusiMG,PerfettiG,AutorinoGL. Pre-liminaryobservationsonthepotentialroleofsomemammalianreservoirsof Toscanavirus.In:Internationalmeetingonemergingdiseasesandsurveillance 2007.2005.
[14]CalisherCH,WeinbergAN,MuthDJ,LazuickJS.ToscanavirusinfectioninUnited StatescitizenreturningfromItaly.Lancet1987;1(8525):165–6.
[15]SchwarzTF,GilchS,JagerG.Travel-relatedToscanavirusinfection.Lancet 1993;342(8874):803–4.
[16]BraitoA,CorbisieroR,CorradiniS,MarchiB,SancascianiN,FiorentiniC, Ciu-foliniMG.EvidenceofToscanavirusinfectionswithoutcentralnervoussystem involvement:aserologicalstudy.EurJEpidemiol1997;13(7):761–4. [17]ValassinaM,ValentiniM,PuglieseA,ValensinPE,CusiMG.Serologicalsurvey
ofToscanavirusinfectionsinahigh-riskpopulationinItaly.ClinDiagnLab Immunol2003;10(3):483–4.
[18]TerrosiC,OlivieriR,BiancoC,CellesiC,CusiMG.Age-dependentseroprevalence ofToscanavirusincentralItalyandcorrelationwiththeclinicalprofile.Clin VaccineImmunol2009;16(8):1251–2.
[19]DiNicuoloG,PaglianoP,BattistiS,StaraceM,MininniV,AttanasioV,etal. ToscanaviruscentralnervoussysteminfectionsinsouthernItaly.JClin Micro-biol2005;43(12):6186–8.
[20]CalamusaG,ValentiRM,VitaleF,MamminaC,RomanoN,GoedertJJ,etal. SeroprevalenceofandriskfactorsforToscanaandSicilianvirusinfectionina samplepopulationofSicily(Italy).JInfect2012;64(2):212–7.
[21]ColombaC,SaporitoL,CiufoliniMG,MarchiA,RotoloV,DeGraziaS,etal. PrevalenceofToscanasandflyfevervirusantibodiesinneurologicalpatients andcontrolsubjectsinSicily.NewMicrobiol2012;35(2):161–5.
[22]SoldateschiD,dalMasoGM,ValassinaM,SantiniL,BianchiS,CusiMG. Lab-oratorydiagnosisofToscanavirusinfectionbyenzymeimmunoassaywith recombinantviralnucleoprotein.JClinMicrobiol1999;37(3):649–52. [23]BraitoA,CorbisieroR,CorradiniS,FiorentiniC,CiufoliniMG.Toscanavirus
infectionsofthecentralnervoussysteminchildren:areportof14cases.J Pediatr1998;132(1):144–8.
[24]Charrel RN, Gallian P, Navarro-Mari JM, Nicoletti L, Papa A, Sanchez-Seco MP,etal. Emergenceof ToscanavirusinEurope.EmergInfect Dis 2005;11(11):1657–63.
[25]ErgunayK,LitzbaN,LoMM,AydoganS,SayganMB,UsD,etal.Performanceof variouscommercialassaysforthedetectionofToscanavirusantibodies.Vector BorneZoonoticDis2011;11(6):781–7.
[26]MaguranoF,NicolettiL.HumoralresponseinToscanavirusacuteneurologic diseaseinvestigatedbyviral-protein-specificimmunoassays.ClinDiagnLab Immunol1999;6(1):55–60.
[27]Collao X, Palacios G, Sanbonmatsu-Gamez S,Perez-Ruiz M,Negredo AI, Navarro-MariJM,etal.GeneticdiversityofToscanavirus.EmergInfectDis 2009;15(4):574–7.