Ph.D. School in Engineering “L. Da Vinci”
PhD Thesis
PhD course on Automatic, Robotics and Bioengineering
XXVI (2011-2013)
SSD: ING-INF/06
Person-centric decision support systems
and ontologies: advanced architectures
for the next generation of clinical
applications
Tutor: Prof. Giovanni Pioggia
Student: Daniele Corda
1
Summary
Introduction ... 6
Chapter 1 New Concept of DSS ...10
1.1 Introduction ...10
1.2 The Concept ...12
1.3 An Adapted Architecture for Elderly People ...15
Chapter 2 Heart Diseases ...17
2.1 The Heart ...17 2.1.1 Introduction ...17 2.1.2 Electrocardiogram ...22 2.1.3 HRV Assessment ...25 2.2 Heart Failure ...27 2.3 Stroke ...30
Chapter 3 A Wearable System for Heart Monitoring ...33
3.1 Introduction ...33
3.2 The Architecture ...34
3.3 Sensor Side ...38
3.3.1 State of Art...38
3.3.3 The Hardware ...47
3.3.2 The Chest Belt ...50
3.3.3 The Firmware ...54
3.4 Mobile Side ...58
3.5 Server Side ...63
3.6 Results ...66
3.7 Conclusions ...69
Chapter 4 Recognition of Elementary Upper Limb Movements ...70
4.1 Introduction ...70
2
4.3 Materials and Methods ...75
4.3.1 Movement Selection ...75
4.3.2 Sensor Selection and Placement ...78
4.3.3 Algorithm Design ...79 4.4 Results ...89 4.5 Conclusions ...91 Final Remarks ...93 Publications ...95 References ...97 Acknowledgements ...103
3
Index of Figures
Figure 1. Statistics about the mortality ...11
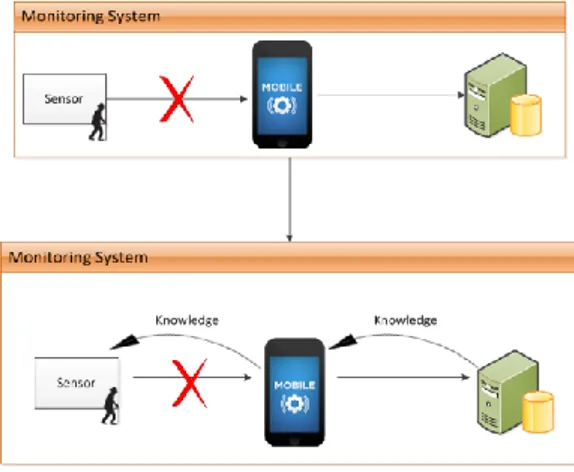
Figure 2. The change of the DSS concept. The old concept on the top and the new one on the bottom ...12
Figure 3. New approach ...14
Figure 4. The real problem during monitoring of physiological parameters in elderly people ...15
Figure 5. Important aspects for an Hyper Ontology ...16
Figure 6. The heart ...18
Figure 7. Cardiovascular system ...19
Figure 8. Myocardial conduction ...20
Figure 9. ECG ...22
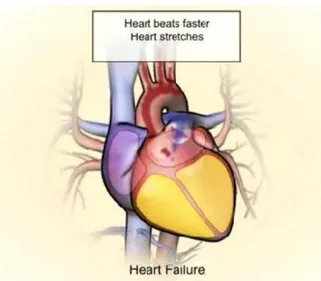
Figure 10. Hypertrophy during heart failure ...28
Figure 11. Stroke disease ...30
Figure 12. The Architecture ...34
Figure 13. The mobile pervasive architecture ...37
Figure 14. VS100 ...38
Figure 15. VS100 placement ...40
Figure 16. CardioPatch ...40
Figure 17. CardioSystem ...41
Figure 18. Set-up sensors ...42
Figure 19. Radio module ...42
Figure 20. ECG module ...43
Figure 21. BluECG device ...43
Figure 22. ECG belt ...44
Figure 23. BluECG device with smartphone ...44
Figure 24. BioPatch device ...45
4
Figure 26. MicroSD module ...48
Figure 27. Connector to expand the sensor board ...49
Figure 28. Customized wearable ECG chest strap ...51
Figure 29. Components to form an executable ...54
Figure 30. NesC Application ...54
Figure 31. The sensor capabilities ...56
Figure 32. Packet format ...57
Figure 33. Smartphone application ...58
Figure 34. Server side architecture...63
Figure 35. It shows the comparison of RMSSD between the Control group and the Patients ...68
Figure 36. Basic steps of task detection using sensor orientation ...79
Figure 37. The X, Y, Z axes accelerometers are shown with red, blue and green arrows respectively. ...79
Figure 38. Customised sloped wedges having inclination of 10°, 20°, 30° and 40°. ...80
Figure 39. Accelerometer calibration curve showing a plot against the theoretical acceleration vs. the measured output. ...81
Figure 40. Standard orientations of the sensor module to recognize the 3 tasks. ...83
Figure 41. Transition from Position1 (left) to Position4 (right) denoting a drinking activity, Task B ...86
Figure 42. Transition from Position1 (left) to Position6 (right) denoting a rotation of the arm, Task D ...86
5
Index of Tables
Table 1. Sensor requirements ...51
Table 2. Possible uses of the single-lead ECG system. ...53
Table 3. Command list ...57
Table 4. Sensitivity and specificity extracted from collected ECG signals ...66
Table 5. Results obtained from a features extraction (standard deviation of each features inside brackets) ...67
Table 6. Use case: activity list ...77
Table 7. Calibrated coefficients for the tri-axial accelerometer ...82
Table 8. Sequence transition and corresponding task ...85
Table 9. Pseudo code for task recognition ...88
Table 10. Recognition of trials by healthy subjects ...90
6
Introduction
Today the importance of knowledge for medicine as a task requiring computer support in clinical and applied research receives a great emphasis. As pointed out by several researchers, although there is the need of a personalized treatment, nowadays there is a little knowledge about how to identify the most suitable treatment or integration of treatment for each specific patient. There is a need to bring the assessment and the therapy out of the clinical environment and develop a patient-centric home-based intervention solution requiring a minimal human involvement and therefore extremely cost effective. The strict focus on the medical setting has now broadened across the healthcare spectrum, and instead of artificial intelligence systems, it is typical to describe them as Clinical Decision Support Systems (CDSS). Pattern classification, expert and artificial intelligence systems, better described as knowledge-based CDSS, are today found an effective application and represent in perspective a real technological breakthrough. A CDSS consists of the objective and quantitative assessment of clinical data; the decision support for treatment planning through pattern classification algorithms; and the provision of warnings and motivating feedback to improve compliance and long-term outcome. Developments in computational techniques including clinical decision support systems, information processing, wireless communication and data mining hold new premises in personal health systems. Pervasive healthcare architectures are today found an effective application and represent in perspective a real technological breakthrough promoting a paradigm shift from diagnosis and treatment of patients based on
7
symptoms to diagnosis and treatment based on risk assessment. Such architectures must be able to collect and manage a large quantity of data supporting the physicians in their decision process through a continuous pervasive remote monitoring model aimed to enhance the understanding of the dynamic disease state and personal risk. The medical knowledge is frequently updated and re-evaluated comprising new risk factors identification, new drugs and diagnostic tests, new evidences from clinical studies. The challenge faced today is to incorporate the most recent and evidence-based knowledge into personal health systems and to transform collected information into valuable knowledge and intelligence to support decision making. Several expert systems tailored to specific diseases are nowadays available in clinical research, often covering the topics addressed by European priorities. Technology can play a key role to gain the continuity of care and a person-centric model, focusing on a knowledge-based approach integrating past and current data of each patient together with statistical evidences. In currently applied care practices, the emergence of clinical symptoms allows a disease to be discovered. Only then, a diagnosis is obtained and a treatment is provided. Currently, different healthcare practice models are used. In some models, the Hospital is the core of the care and any level of technology available at the patient site may help in providing information useful for both monitoring, early diagnosis and preventive treatments. In other models dedicated call centres or point of care act as an intermediary between hospital/heath care professional and patients. Many of the solutions available today on the market follow the above-mentioned model and call centre services or point of care are used by the patients just as a complement to the hospital-centred healthcare services. In a more advanced concept focused on
8
the empowerment, the ownership of the care service is fully taken by the individual. This model is suitable for any of the stages of an individual’s care cycle, providing prevention, early diagnosis services and personalized chronic disease management. Under this model, the technological innovations can help each persons to self-engage and manage his/her own health status, minimizing any interaction with other health care actors. Solutions fully led by the patients are the overwhelming majority of those developed by research efforts covering chronic disease management, lifestyle management and independent living. Even if, in the clinical practice this model has not been yet implemented, it can be considered as a target to be reached achieving at the same time the empowerment of the users and the reduction of workload and costs, preserving the quality and safety of care. However, this model often fails to give the expected results and research is under development. This happens for a series of concomitant causes, ranging from legal and societal obstacles, to the issues to be tackled before these wearable devices are ready for general use, up to the inappropriate use of the decision support system, as well as to win the scepticism of many healthcare professionals. Wearable devices need to be non-intrusive, easy to use, comfortable to wear, efficient in power consumption, privacy compliant, with very low failure rates and high accuracy in triggering alarms, especially if used for diagnostic purposes. The decision support system must infuse clinical knowledge into methodology and technology, thus enhancing the reliability of high-level processing systems customized to his/her personal needs represents the next critical step. The currently used approaches are only based on values of health-related parameters, often monitored instantaneously during a check-up. Moreover, the correlation across physiological, psycho-emotional, environmental and
9
behavioural parameters are poorly explored, because the diagnosis of a disease largely depends on the experience of the individual doctors.
10
Chapter 1 New Concept of DSS
1.1 Introduction
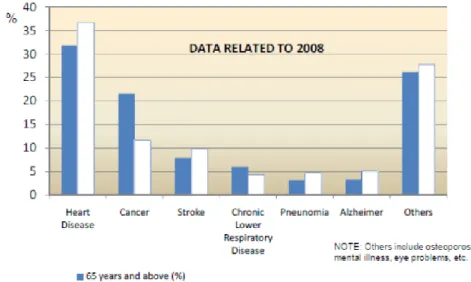
As effect of the increased longevity and reduced birth-rate, the older population is growing at a considerably fast rate. This rapid expansion of the older population affects practically all the regions of the world and is increasing: by 2020 the 65+ population will represent 25% of the overall population in Europe. The ageing of the population is changing also the workforce scenario: currently in Europe the ratio between working people and retired ones is equal to 4:1 but analysts expect a drastic reduction of this ratio up to 2:1 in 2050. Healthcare and Pension systems are struggling to cope with additional demand also in consideration that age and disability are strongly correlated: around a fifth of people over 50 experience severe vision, hearing and dexterity problems. The profound, pervasive and enduring consequences of ageing population present enormous challenges as well as enormous opportunities for Information and Communication Technology. A typical example is the Internet that has become an enabler of social inclusion. In Figure 1 is possible to see what is the incidence of the mortality caused by many factors, in particular there is a preponderance of heart disease.
11
Figure 1. Statistics about the mortality
For this reason my PhD aim has been the research of strategies to prevent heart disease (screening point of view) and to increase the quality of life for elderly people affected by these kind of problems (rehabilitation point of view). In particular the aim of my PhD was the development of novel architectures combining the monitoring of health parameters and the expert biomedical knowledge with the patients’ psychological profile, as well as their social and environmental context, to efficiently diagnose, treat or manage diseases in several applications.
12
1.2 The Concept
The considerable progress in the field of electronics and informatics technology during these last few years have made sure that the DSS (Decision Support System) idea is changing. The concept is going from a server centric view (server as a central node), at least from the algorithmic point of view, to a distributed DSS view, where the algorithmic intelligence is present at the sensor level, at the intermediate level (e.g. on PC or Smartphone) and at a server level.
13
Moreover a new architecture means the joint between screening and rehabilitation techniques in order to have a complete view about the situation of the patient to customize treatment.
Screening is a process of identifying apparently healthy people who
may be at increased risk of a disease or condition. They can then be offered information, further tests and appropriate treatment to reduce their risk and/or any complications arising from the disease or condition.
Rehabilitation is the process of helping an individual achieve the
highest level of independence and quality of life possible - physically, emotionally, socially, and spiritually. Rehabilitation does not reverse or undo the damage caused by a stroke, but rather helps restore the individual to optimal health, functioning, and well-being. Rehabilitate (from the Latin "habilitas") means "to make able again."
In particular the screening point of view is changing, as it is possible to see in Figure 3.
14
Figure 3. New approach
Actually the sanity purpose should be to do screening, to find out a pathological state before the symptoms appearance.
15
1.3 An Adapted Architecture for
Elderly People
I started my research activities within an European project (OASIS), where I collaborated for the development and integration of a wearable architecture to monitor elderly people during real life. At the beginning of my work I noted there was a big problem to make elderly people really able to use all technologies, useful to obtain the results in according to the goal of the project. This is real because often, the use of Smartphones, or other technologies, is not a common attitude for an elder. For this reason I understood that I had to focus my research attention to solve this problem. How can I solve it? I thought to work out it simplifying the DSS model (Server Side) in order to have the possibility to transfer the knowledge from the server to the sensor. In this case I can obtain a wearable system that basically needs only a sensor to work (to do screening).
16
To improve the life quality for elderly people it is important to develop an informatics tool considering following aspects:
Independent Living Applications
Mobility Applications
Smart Workplaces Applications
Socialisation
Figure 5. Important aspects for an Hyper Ontology
The goal of my research activity was to develop an architecture able to combine these aspects as better as possible. I thought to joint the concept of Independent Living Applications, Mobility Applications, Smart Workplaces Applications in one architecture, thanks the electronic world, that includes the use of Smartphones, Tablets and so on.
17
Chapter 2 Heart Diseases
2.1 The Heart
2.1.1 Introduction
The heart, placed in the central area of the chest (between the two lungs), is a hollow muscular organ arranged between the venous and the arterial section of the cardiovascular circle. It’s a pump capable of producing a blood pressure sufficient to ensure the circulation of blood throughout the body, by means of an alternation of contractions (systole) and relaxations (diastole). It consists of 4 cavities:
2 upper (left and right atrium)
18
Figure 6. The heart
The left side of the heart, in which arterial oxygenated blood flows, is separated from the right side , in which venous carbon dioxide rich blood flows, by a robust vertical wall , the septum . Each of the two atria is superimposed on the respective ventricle , with whom he communicates through an atrioventricular hole. The right atrioventricular hole is equipped with a valve, the tricuspid valve to the left of another , the bicuspid or mitral valve . The valves , closing , prevent the backflow of blood from the ventricle to the atrium during systole. The state of the valves depends only thanks to the difference in pressure between the chambers. If the atrial pressure is greater than ventricular, the valves are open and allow the filling of the ventricle , in the opposite case are closed preventing the return of blood in the atrium during ventricular contraction. The same purpose about the semilunar valves , pulmonary and aortic, placed between the ventricles and the great arteries (pulmonary artery and aorta). The semilunar valves make unidirectional the flow of blood to the pulmonary artery and the aorta ,
19
because they prevent the backflow of blood into the respective ventricles during the relaxation phase of the myocardium. There are no valves in the entrance of the atria. The blood flow follows a well-defined path :
The right atrium receives blood from the body, it moves to the right ventricle
The right ventricle pumps it into the lungs to receive oxygenated blood
The oxygenated blood returns from the lungs to the left atrium
The blood passes into the left ventricle which pumps it to the rest of the body
Figure 7. Cardiovascular system
The heart is an organ composed primarily of muscle and a nervous tissue. The muscle tissue is formed by three tunics one inside the other : the epicardium , myocardium and endocardium, wrapped by a thin membrane called pericardium. The myocardium supports the pumping function of the blood
20
(mechanical activity) and is endowed with the capacity of self-contraction (electrical activity). The myocardium is formed by a system of cells (pacemaker) and fibres , said " conduction system " , in which automatically, for spontaneous activity , are formed electrical stimuli that , spreading into muscle tissue , stimulate it to contract. The heart is the only organ that has this ability contractile own. Normally the stimulus arises in the sinoatrial node , which imposes its rhythm to the entire cardiac muscle , with a heart rate of about 70-75 beats per minute . The stimulus from the sinoatrial node reaches the atrial musculature and , subsequently , the atrioventricular node : from here passes into the bundle of His , in its branches left and right , up to small branches which penetrate throughout the myocardium (the Purkinje fibres).
Figure 8. Myocardial conduction
The transmission of pulses and the subsequent myocardial contraction is not a random event, but adjusted in such a way as to generate the so called cardiac
21
cycle (alternating rhythmic contraction or systole and diastole or relaxation). The electrical phenomena (currents) that originate in the heart are transmitted throughout the body, which is a good conductor of electricity. These currents are recorded using the Electrocardiogram (ECG) through a non-invasive measurement. This measure allows to obtain a track composed of the P waves, QRS and T, each of which identifies a different phase of the cardiac cycle.
22
2.1.2 Electrocardiogram
The electrocardiogram (ECG) is a recording of the electrical activity of the heart that occurs in the cardiac cycle.
Figure 9. ECG
The principle on which the measurement of electrical activity of the heart is based is purely physiological: the onset of the impulses in the myocardium leads to the generation of potential differences, which vary in space and time and that can be recorded through the electrodes. The registration of potential difference by electrodes placed on the body surface occurs thanks to the conductivity of the interstitial fluids of the human body. The electrocardiogram is the easiest, least expensive and most convenient way to
23
see if the electrical activity of the heart is normal. The normal ECG has a characteristic that varies only in the presence of problems. The track is characterized by several traits called waves, positive and negative, that are repeated at each cardiac cycle . The first derivation or D1 is obtained by taking the difference of potential between the two electrodes placed on the right arm and the left arm: D1 = LA – RA.
P wave: it is the first wave that is generated in the cycle , and
corresponds to the depolarization of the atria. It is small in size because the contraction of the atria is not so powerful . Its duration varies between 60 and 100 ms.
QRS complex: it is a set of three waves and corresponds to the
depolarization of the ventricles . The Q wave is negative and small in size , and corresponds to the depolarization of the interventricular septum , the R is a high positive peak, and corresponds to the depolarization of the apex of the left ventricle , the S wave is also negative and small in size, and corresponds to the depolarization of the baseline and rear regions of the left ventricle . The duration of the entire complex is between 60 and 90 ms . In this interval, the atrial repolarization also occurs but is not visible because masked by ventricular depolarization .
T wave: it represents the repolarization of the ventricles. It is not
always identifiable , because it can also be of very small value.
Wave U: it is a wave that is not always possible to appreciate in a track,
24
The second derivation or D2 is obtained by taking the difference of potential between the electrode of the right arm and the left leg: D2 = LL – RA. The third derivation or D3 is obtained by taking the difference of potential between the electrode of the left arm and the left leg: D3 = LA – LL.
25
2.1.3 HRV Assessment
Heart rate has a prognostic importance and the knowledge of the mean, minimum (resting) and maximal (exercise) heart rate may help in the decision making for optimal therapeutic strategies. But another important aspect of ECG monitoring is represented by the assessment of heart rate variability (HRV), which can be extrapolated from ECG. HRV helps to identify the neuro-hormonal balance which has significant prognostic implication. It reflects behaviour of both parts of autonomous nervous system: sympathetic and parasympathetic. It is widely used for quantifying neural cardiac control [1], and low variability is particularly predictive of death in patients after myocardial infarction [2]. Infact, patients with lower HRV values show the highest mortality rate compared with patients with higher HRV values. A number of earlier studies of HRV have shown significant prognostic information in chronic heart failure (CHF). The United Kingdom Heart Failure Evaluation and Assessment of Risk Trial [3](in 433 outpatients) found that reduced SDNN (SD of the normal-to-normal R-R interval) from 24-hour Holter ECG predicted death from progressive heart failure but failed to predict sudden cardiac death. It might be expected that increased sympathetic activity would be accompanied by a relative predominance of LF oscillations in frequency-domain analysis of HRV [4]. However, both increased [5] and reduced [6] LF power were found to be associated with an increased risk of cardiac death. Data from Galinier et al. [7] showed that reduced daytime LF power from 24-hour Holter recording independently and significantly predicted sudden death, although very few other parameters were included in
26
the analysis. La Rovere et al. [8] demonstrate how reduced 24-hour time and frequency-domain measures of HRV identify CHF patients at increased risk of death. In the present study is shown that a simple bedside ECG recording of less than 10 minutes of duration and an LF power analysis of HRV obtained during controlled breathing provides additional important prognostic information. Moreover Vazir et al. [9] sustain that in the majority of congestive heart failure patients with mild-to-moderate symptoms, the analysis of nocturnal heart rate variability by spectral analysis is a quick, easy and a promising screening tool for sleep-disordered breathing. Setting the percent very low frequency index at 2.23% provided a high negative predictive value that was necessary for a rule-out test for sleep-disordered breathing both for central and obstructive sleep apnoea. Finally several recent studies demonstrates that HRV parameters continuously measured from invasive and non-invasive cardiac devices reduce patients’ mortality and hospitalization risk [10] [11] [12] [13].
27
2.2 Heart Failure
The term " Heart Failure” means a condition that occurs when the heart , and in particular the left ventricle , loses the normal ability to pump blood to maintain the body's vital functions , working with lower efficiency. It is a chronic progressive systemic disease in which , following a cardiovascular dysfunction , it determines the neuro humoral activation, with consequent involvement of all organs and systems. The neuro humoral activation represents the pathophysiological mechanism of the most common symptoms of heart failure : low cardiac output , hydro saline retention , vasoconstriction. They are so different to create alterations in the arterial and venous circulation, which further aggravates the condition of the heart. The most common cause is myocardial infarction , that causes the replacement of heart muscle tissue with scar tissue . Initially, the amount of blood pumped from the heart to the rest of the body is reduced, while the one that returns to the heart from the body encounters a resistance greater than normal . This not only makes people feel very tired because it decreases the supply of oxygen to the muscles, but it also brings the kidneys to retain water and minerals, causing an excess of fluid in the body that leads to further fatigue infarction. Consequently , the increase in venous pressure causes an output of blood from the vessels, causing edema to the lungs or to the lower limbs . Usually heart failure is a phenomenon that develops slowly , so it may take years before obvious symptoms emerge and action can be taken . Another common cause of heart failure is high blood pressure that causes the thickening of the muscle of the left ventricle , leading to the loss of flexibility and decreased ability to
28
pump blood. It is important to identify any precipitating factor in order to establish the optimal treatment of heart failure .
Figure 10. Hypertrophy during heart failure
When you manifest heart failure , the heart is unable to meet its functions , being very tired as a result of the events listed above. From the pathophysiological point of view , the failure may have originated from a worsening of systolic or diastolic function , or more often , by a deterioration of both . In the case of systolic dysfunction , stroke volume is reduced, with a consequent decrease in the rate. In order to preserve the latter , the heart can react with three failure mechanisms : the first is the increase in blood return (preload) , which induces a greater contraction of the sarcomeres , the second mechanism consists in the release of catecholamine, which may increase cardiac output by increasing the frequency of the beats , and finally , the heart muscle can hypertrophy and ventricular volume may increase. Because the
29
heart is already weak , these attempts of compensation are not sufficient and cause a deterioration in the long term , of cardiac muscle .
30
2.3 Stroke
Figure 11. Stroke disease
A stroke occurs when blood flow to a part of the brain stops. A stroke is sometimes called a "brain attack". If blood flow is cut off for longer than a few seconds, the brain cannot get blood and oxygen. Brain cells can die, causing lasting damage.
There are two major types of stroke:
Ischemic stroke
Hemorrhagic stroke
Ischemic stroke occurs when a blood vessel that supplies blood to the brain is blocked by a blood clot. This may happen in two ways:
31
A clot may form in an artery that is already very narrow. This is called a thrombotic stroke.
A clot may break off from another place in the blood vessels of the brain, or from some other part of the body, and travel up to the brain. This is called cerebral embolism, or an embolic stroke.
Ischemic strokes may be caused by a sticky substance called plaque that can clog arteries. A hemorrhagic stroke occurs when a blood vessel in part of the brain becomes weak and bursts open. This causes blood to leak into the brain. Some people have defects in the blood vessels of the brain that make this more likely. These defects may include:
Aneurysm
Arteriovenous malformation (AVM)
High blood pressure is the main risk factor for strokes. The other major risk factors are:
Atrial fibrillation
Diabetes
Family history of stroke
High cholesterol
Increasing age, especially after age 55
32
Stroke risk is also higher in:
People who have heart disease or poor blood flow in their legs caused by narrowed arteries
People who have unhealthy lifestyle habits such as smoking, high fat diet, and lack of exercise
Women who take birth control pills (especially those who smoke and are older than 35)
33
Chapter 3 A Wearable System
for Heart Monitoring
3.1 Introduction
There is an increasing need to find new ways of managing the European healthcare models due to the demographic and socio-economic challenges that result from the fast ageing of the population. In particular, the increasing number of elderly people directly entails an increasing number of patients with cardiovascular diseases. This type of patients, usually with limited physical activity, remains at home, outside the hospital environment and their health status continues to worsen with episodes of crisis leading to acute deterioration. These episodes, which require emergency and long-time hospital admissions, are always preceded by noticeable changes in several physiological parameters. In this context, accurate and reliable remote monitoring solutions take a main role in order to predict cardiovascular risk of patients and improve their quality of life. To reach this goal in this chapter a prototype of an implemented non-invasive wearable sensor platform for cardiac monitoring is presented and described. The introduction is focused on the applications and clinical scenarios of ECG monitoring with one single lead and the importance of heart rate variability (HRV) analysis as predictive marker
34
for the patient’s risk clusterization to determine the best medical managing strategy.
3.2 The Architecture
Personal Sensing Platform Smartphone Central Server Chest Belt ECG Sensor Local DataBaseProcessing RealTime DSS (Decision Support System) Decision Visualization Module Comunication Module
Figure 12. The Architecture
Many projects have recently addressed the development of protocol stacks, security solutions, and middleware layers for large scale wireless sensor networks. The focus has been on low power HW and low energy consuming protocol stacks, secure wireless communications for embedded devices, seamless integration of heterogeneous sensor nodes and wireless devices. A major challenge in next generation WSNs will be the integration and cooperation of heterogeneous devices (heterogeneous sensor devices, PDAs, mobile phone etc.). Some project aim to provide an adaptive middleware
35
platform and a common language that will simplify the application creation process on heterogeneous technologies. Security is a key element of business solutions often neglected in WSN projects. Some investigations on the middleware and protocol parts have been done too. This comprises work on security configurations, secure protocols for routing and key distribution etc. However, current solutions still have limits when applied to personal health management. Network protocols are not holistically designed and optimized and (above all) often fail to meet the requirements of applications where security is an issue. Moreover, there is a need for lightweight network management solutions that can be adopted to monitor systems made of resource constrained embedded devices. The communication protocol stack developed will solve many of the limitations of currently available solutions (in terms of energy, efficiency, security and reliability of the communications, QoS support, support for accurate localization and tracking of equipment/people). In particular, I collaborated to design and implement:
• Secure, reliable protocol stacks which are suitable for embedded devices and can timely deliver information
• Solutions that require extremely low energy
• Support for end to end reliability, security and QoS in a scenario made of heterogeneous devices and technologies
• Tools and methodologies to support deployments of the sensor nodes, easy programmability and re-programmability
• Lightweight network management solutions
• Middleware layer for easy service provisioning using the WSN functionalities
36
From a general point of view, a mobile pervasive architecture consists of different wireless modules cooperating in order to perform data acquisition from multiple sensors, data analysis and decision through several techniques and data redirection and feedbacks. The architecture here proposed addresses the design of a flexible instrument for data acquisition, management, elaboration and decision suitable for those systems which are equipped with distributed remote wearable devices, where a particular attention is paid to
the heterogeneous medical information flow and inter-process
communication. Moreover, the possibility to operate in real time imposes critical efficiency requirements to each single module. The core of the architecture is the Smartphone which collects data from the Personal Mobile Sensing Platform using a configurable time resolution and dedicated Bluetooth communication channels. A data pre-processing step is performed on-board, so that the wireless communication with the Smartphone is significantly reduced. The Smartphone is able to integrate the time-aligned wearable sensor information and to store relevant data in its own local DataBase (DB). The Smartphone performs a provisional analysis of device-mediated responses (Lite Processing), being able to take into account context information (GPS, motion activity) and physiological data (e.g. hearth rate, heart rate variability) to obtain a provisional score (Mobile Reasoning Module). The provisional score triggers a more accurate analysis and/or perform the local feedback strategy. In the case of a provisional score higher than a fixed (configurable) threshold, the Smartphone is able to establish a connection with the central DB and to upload the collected data for further and more accurate analysis. The central DB I/O communication layer is implemented through a Web Services Description Language (WSDL) interface according to a standard protocol. The
37
WSDL interface design pays attention to the management and the synchronization of data and processes.
38
3.3 Sensor Side
3.3.1 State of Art
VitalSens100
This device is the product that connects to the whole system of Intelesens about the monitoring of vital activities.
Figure 14. VS100
VS100 facilitates the measurement and communication of ECG, Heart Rate, surface temperature of the skin and movements.
The device can be configured for different modes of data collection:
• Periodic data transfer via Bluetooth • Live streaming of data via Bluetooth
The transmitted data can be viewed in real time or recorded for further analysis by specialized doctors. Key features of the device of Intelesens in addition to those mentioned above are the fact of having separate sensors
39
with a replaceable electrode Plug and play for multiple measurements, the miniaturization of wireless sensors for body easy to wear and can be applied directly from the patient with a compact design and light type electrodes with non-irritating but especially the portability of the main station with rechargeable lithium-ion battery. Vitalsens100 is designed to provide wireless ECG, heart rate, temperature of the surface of the skin and monitoring of activities. It was designed to be quickly added or integrated to medical devices or more complex systems, such as removing cables from hospital beds and equipment attached to them, or create from scratch monitoring situations without hindrances to the staff. It is also increasingly active research and innovation in areas of connection between the various types of electrocardiograms. Using this platform, the path between the doctor-patient relationship is much faster and safer compared to other devices. Consists of five main parts, the VS100 is an ultra-compact and easy use in any field, whether hospital or home. The Bluetooth transmitter part is the generation protocol with EDR Class II traveling in power 2.5 mW and 4 dBm which support the device up to about 10 meters away. The electrodes with an innovative design are in the form of patches that last up to 24 hours, they are disposable type and not irritable, very easy to wear for any patient without particular care. As regards the part for the ECG and Heart Rate there is a device of II Lead type with sampling frequency of 360 samples per second with 12-bit of resolution. There are also three-axis accelerometer, classic X, Y, Z, with 40Hz/160 Hz of sample rate and 16 bit of resolution. Finally, a temperature sensor integrated in the electrode surface with sample rate of 10 samples per second with 12-bit of resolution and temperature range from 20 degrees to 45 degrees [14].
40
Figure 15. VS100 placement
CardioPatch
Figure 16. CardioPatch
Until now the main problems related to the wireless ECG device were:
Not having wires could cause false alarms
The mobility of the patient was greatly reduced.
The management of these devices needed huge amount of time
41
For these reasons the Novosense projected these sensors designed ultra-thin and ergonomic with wireless technology called CardioPatch. All sensors forming part of a structure called CardioSenseSystem.
Figure 17. CardioSystem
The system, as it’s possible to see in the diagram includes a receiver, the CardioBase, which passes the signal directly to the monitor of the doctor or in a database contained in a data storage provided. Based on three electrodes, this multimedia device should be placed in certain points of the body in order to monitor the electrical activity of the heart. The figure illustrates the specific placement of the sensors.
42
Figure 18. Set-up sensors
We can divide the sensor into two main parts: the radio module and the ECG module. Antenna integrated, radio module type Chipcon CC2420 and MSP430F1612 processor make up the hardware of the transmitter, which is compliant BWSN3 version 1.1 as regards the transmission of the message format. The implementation was made with C code. The ECG module is much simpler and has two main circuits connected directly to the radio module, the ECG signal amplifier and MSP430F1612 processor to manage the data [14].
43
Figure 20. ECG module
BluECG
This electrocardiograph acquires and reproduces the 12 leads electrocardiographic signal, by means of a smartphone.
Figure 21. BluECG device
The smartphone receives the signal as encoded file in a proprietary format and sends it (GPRS / Wi-Fi) to the server. After the signal stored in the database, the server processes the ECG according to the type of management associated with the sender device. The signal is sent to a list of recipients by default, consists of several cardiologists. If you are not answered within a predetermined time, the signal is sent to the next recipient, and so on until you get a response. The patient may receive the diagnosis in real time via e-mail or text message containing the report analysed by the cardiologist. For
44
the recording of the signal, the patient wears a particular band, constituted by the electrodes, of easy application even by unauthorized personnel [15].
Figure 22. ECG belt
45
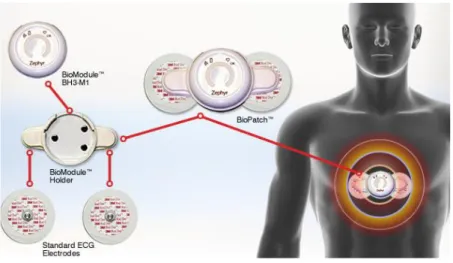
BioPatch
Figure 24. BioPatch device
The BioPatch is an easy way to attach patients to the ZephyrLIFE system. Comfortable and small, the BioPatch attaches to traditional disposable ECG electrodes and allows the BioModule to easily be snapped in [16].
Features:
BioModule unit snaps into the BioModule Holder that attaches to the patient via traditional disposable ECG electrodes
Designed for continuous monitoring
Lightweight and wireless design allows freedom of movement
Long transmission range
Long Battery Life
Water Resistant up to 1m
46
Can be disinfected with standard cleaning agents
Measurements
Heart Rate
R-R Interval
Respiration Rate
47
3.3.3 The Hardware
The device used in the following thesis has been the SHIMMER. This is a small portable device for monitoring in real-time the data acquired.
Figure 25. Hardware It integrates: A three-axis accelerometer A zigbee module A bluetooth module Three LEDs
48
Through the external connector the SHIMMER can be programmed. The reset button allows you to turn on, turn off or reset the device. The LED give feedback about the operation of the device, different colours have different meanings:
Red: the device is damaged or discharge
Yellow: advised to be careful
Furthermore, during the communications (hence the use of zigbee or bluetooth module) the LEDs have the following meanings:
Green: Connection successful
Blinking Yellow: data transfer in progress
This device offers the ability to add external memory (microSD):
Figure 26. MicroSD module
It is also possible to expand the device board to add any characteristics or stages of adaptation of the signal, this is possible using a special connector.
49
Figure 27. Connector to expand the sensor board
The microprocessor present in SHIMMER is a MSP430F1611 (produced by Texas Instrument), this belongs to, as the name suggests, the family of MSP430 microcontrollers composed of several devices with different types of peripherals targeted for various applications. The 16-bit RISC architecture, based on the low power consumption makes it ideal for its use of portable devices in that it allows a longer battery life. In particular, the MSP430F1611 has two 16-bit internal timer (A, B), 12-bit A/D converter, USART serial communication interface configurable in synchronous or asynchronous mode with 48 I/O pins [17].
The salient features of the microcontroller:
10Kbytes of RAM, 48Kbyte of Flash
8MHz Clock
2 DAC outputs
50
3.3.2 The Chest Belt
Presently, egocentric sensing systems consisting of biomimetic wearable suits (BWSs) for the unobtrusive biomonitoring of body-kinematics and physiological and behavioural signals are continuously improving. Integrated wearable systems are able to transduce heart rate and electrocardiographic signals (ECG). I optimized the design of a chest strap embodying electrodes, the related electrical connections and a dedicated portable integrated electronic board placed at the level of the thorax. The chest strap is mainly made of flexible biocompatible elastomer, cotton and elastan; it is fully washable and guarantee an optimal and comfortable contact between the strap and the thorax adapting itself to the body shape. The chest strap registers the heart's electrical signal mimicking the bipolar lead of the classical ECG measurement configuration. The system is able to visualize the normal sinus rhythm, arrhythmias and extrasystoles (a premature contraction of one of the chambers of the heart), and to assess heart rate (HR) and heart rate variability (HRV) through dedicated algorithms. I intended to extract time-domain and frequency-time-domain features of ECG signals through advanced signal processing techniques in order to localize the sympathetic and parasympathetic nervous system activities associated with different frequency bands, quantitatively assessing HRV signals by means of power spectral analysis. The powers of high frequency (HF) and low frequency (LF) components of HRV, as well as the LF/HF ratio, allow cardiac vagal and sympathetic activities as markers of autonomic interaction to be estimated.
51
The sensor I used to do this research activity was the commercially available Shimmer ECG wireless sensor module with the following requirements:
Table 1. Sensor requirements
The wearable system is composed by:
The ECG sensor
A Chest belt
A Smartphone
52
The sensor is easily applied to the chest belt that should be placed in the patient's diaphragmatic zone. The Smartphone is able to communicate with the Server, this is important to collect and elaborate the ECG data to extract important features to do a research analysis. Obviously, it should be remarked that not every problem in cardiac field should be detected and solved by using the simple single-lead ECG, otherwise it shouldn’t have sense to use traditional 12-lead ECG tools. In fact, single-lead systems are not capable to prevent stroke, one of the most burdensome problems concerning cardiac world, and also they can’t prevent myocardial ischemia. Anyway, a general overview of the possible employments of the single lead ECG wearable system [18] [19] is shown in the Table 2.
53
Table 2. Possible uses of the single-lead ECG system.
Use Proposal YES NO
Post-Acute Event Rehabilitation (CHF,
etc.) X
Pharmacological Response Evaluation
and Monitoring (CHF, etc.) X Sinus tachycardia / bradycardia X
Supraventricular, ventricular
arrhythmias X
Cardiac events during selected activities (sleeping, eating, exercise
etc. )
X
Cardiac events during specific symptoms (syncope, dyspnea,
dizziness) X Chronotropic competence X Sympathovagal effects (CHF) X Myocardial Ischemia X Valvulopaties X Pericardial Effusion X Pulmonary Congestion (CHF) X
54
3.3.3 The Firmware
I developed, tested and validated a firmware for the shimmer device using TinyOS, in the language of nesC programming. TinyOS modules are similar to the C source, but the configurations are different. An application is composed of several components connected together to form an executable.
Figure 29. Components to form an executable
55
The nesC files are the following:
Interface StdControl.nc
Module <username> installation> M.nc
Configuration <username> installation> C.nc Example interface:
interface {StdControl result_t command init (); result_t command start (); result_t command stop (); }
Example form: module BlinkM Provides { StdControl interface; } uses { interface Timer; interface Leds; } ... Example configuration: configuration Blink { } implementation {
56 Main components, BlinkM, SingleTimer, LedsC;
Main.StdControl -> SingleTimer.StdControl; Main.StdControl -> BlinkM.StdControl; BlinkM.Timer -> SingleTimer.Timer; BlinkM.Leds -> LedsC; }
I developed a firmware for the sensor for two use cases:
• A real time streaming
• An offline approach, that means the download of ECG data from the sensor to the smartphone thanks the previous storage into an SD card
Both of these use cases mean a daily use during real life.
57
The communication protocol is realized through a serial communication using a historical packet format, very powerful for detecting lost packet because it is check summed and sequenced.
Figure 32. Packet format
The command list is reported in Table 3:
Table 3. Command list
Command function description flow
0x14 Start Logging SD card Device start to acquire and save ECG data
on SD Card and switch Bluetooth OFF. from master to client 0x28 Start download from SD card
Device start to send raw data to the master; this command works only when the Bluetooth is switched ON
from master to client 0x07 Real-time ECG streaming Device start to send real-time ECG data from master to client 0x3C Delete ECG file Device delete ECG file on SDcard from master to client
58
3.4 Mobile Side
Figure 33. Smartphone application
The Sensor Smartphone application enables the user to monitor various physiological parameters such as heart beat, and activity, using their smartphone and a connected sensor. Sensor smartphone can communicate with up to 16 simultaneously functioning wireless, wired or internal sensors, to collect, encrypt and save data locally. The solution can synchronize data with the Sensor Server via secure connections (WiFi, 3G) or work as a stand-alone application. The collected data can be shown in numerical forms or in diagrams with adjustable thresholds and color-coding. The user can set statistic parameters (minimum, maximum, average values,..), list and tweak
59
diagrams on one page (with zoom & pan functionality), in real time (live data) or at a later point (data history). I collaborated to extract features in real time, thanks the computational power of the smartphone. The main time domain feature extracted from the developed ECG chest strap for long-term monitoring of patients are reported below:
• RR mean: It is the standard statistical indicator. The Mean of RR is a parameter of random variable distribution, which is defined as a weighted average of this distribution. The mean of all RR intervals is denumerable by following equation:
∑
where N is the total number of all RR intervals.
• HR mean: It is the mean of heart rate. The Mean of heart rate is similar to RR mean described in subsection
∑
where N is the total number of all RR intervals.
60
𝑀𝑆𝑆𝐷 √
−
∑(
−
)
where N is the total number of all RR intervals in segment.
As regards the study of HRV in the frequency domain, this post elaboration is accomplished with power spectrum analysis, which, in principle, requires rigorous stationary conditions that, in strict terms, are unknown to biology. Thus a practical compromise must be found, and this consists of defining as adequate conditions those characterized by the absence of slow trends or step changes in the tachogram. Using the Power Spectral Density (PSD) we can observe the distribution of power signal in the characteristic band of frequencies. In ECG chest belt I extracted PSD using a parametric approach. This method assumes the time series under analysis to be the output of a given mathematical model, and no drastic assumptions are made about the data outside the recording window. The parametric approach of PSD signal is completely independent of the physiologic, anatomic and physical properties of the biologic system under consideration, but provides a simple input-output relationship of the process (black-box approach). A critical point of this method is the choice of the appropriate model to represent the data sequence. The more general case of the parametric estimator is the autoregressive moving average model (ARMA Auto-Regressive Moving Average), represented by the following linear equation:
61 ( ) − ∑ ( − ) ∑ ( − ) ( )
where w(k) is the white noise input of the system (mean value zero and variance equal to λ2), p and q are, the orders of auto-regressive (AR) and moving average (MA) parts, respectively, and ai and bj are the coefficients. The ARMA model may be reformulated as an AR or MA model where the coefficients ai and bj are, respectively, set to zero. Since the estimation of the AR parameters results in liner equations, the AR model is usually employed in place of ARMA or MA models. An autoregressive process of order p is described by the following equation:
( ) − ∑ ( − )
( )
Z-domain transfer function of the system:
( ) ( )
( ) ( ) − ∑
∏ ( − )
where the coefficients characterize the identification and zm are the poles of the corresponding model. Since the power spectral density of y(k) is:
( ) | ( ( ))| ( )
62
where ΔT is the sampling interval and Py(f) is the spectral density of input power, then it follows that:
( )
| − ∑ |
( )
Looking at the last formula is understood that the estimate of the PSD in the case of autoregressive models, is reduced to the calculation of the AR itself [20]. This assessment can be carried out in various ways, including resolution of equations of Yule-Walker and least squares estimation methods. In particular, the Yule-Walker method involves calculating the autocorrelation values and then solve a system of linear equations for estimating the parameters. The parametric spectral estimation is generally more complex than non-parametric. In addition, it requires an a priori choice of the structure and order of the model of signal generation. From each power spectral estimation, I extracted the spectral indexes in order to evaluate the involvement of autonomic system:
• Total Power (TP) (from 0.03 Hz to 0.4 Hz)
• Low frequency component (LF) (from 0.03 Hz to 0.15 Hz) • High frequency component (HF) (from 0.15 Hz to 0.40 Hz) • Low to high frequency component ratio (LF/HF)
63
3.5 Server Side
Server
Wearable System WSDL Layer
Archive DataBase ECG1 ECG1 Background Migration Process
Figure 34. Server side architecture
Basically the architecture is a client-server system, in particular the client is the smartphone (mobile side) that communicate with the server, able to store and manage all data.
64
• Centralized Resources: the server is at the centre of the network, it can manage common resources for all users, such as a centralized database, to avoid the problems of repetition and contradiction
• Safety best: the number of entry points that allow access to the data is less
• Administration at the server level: the poor importance of the clients in this model, they have less need to be administered
• Network development: thanks to this architecture, you can delete or add clients without disturbing the operation of the network and without major changes
The disadvantages of the client-server architecture are:
• High cost due to the technical nature of server
• Weak point: the server is the only weak point in the client-server network, because the entire network is structured around this
With this architecture the client (Smartphone) can’t directly have the access to the physic Data Base. For this reason the architecture need a WSDL layer, that manages an important role for the security of data. In this way, the client communicates with the WSDL that provides to store data into Data Base. This huge amount of data is available to be elaborated, maybe for a feature extraction to investigate in term of research.
The benefits of the WSDL layer are:
• WSDL presents the architectural features of many other XML-based languages were born recently
65
• The language reference integrates with existing standards, avoiding to redefine what has already been defined: WSDL prefers the use of XML Schema to the type system and the definition of SOAP messages • The language is extensible
• WSDL tries to separate out "abstract" description of a service than "concrete" that bind to specific network protocols
• The same service may have different implementations, based on the same abstract description
• The abstract descriptions can be reused, all or in part, for the creation of new services
The disadvantages of the WSDL layer are:
• Performance (in the XML serialization / deserialization, for high piers of data, reduces the speed of the applications)
66
3.6 Results
The first part of the analysis was useful in order to validate the wireless ECG system and to investigate the feasibility of using the sensor in mobile environment. The algorithm has been assessed on the signal collected from the healthy subjects wearing both ECG chest strap and ELA Holter during working activities. In Table 4 are shown the results of the evaluation of the 10 ECG signals collected and analysed with the developed algorithm.
Table 4. Sensitivity and specificity extracted from collected ECG signals
Tape N° Total Beats FN (beats) FP (beats) Sen (%) Spec(%)
1 2273 0 0 100 100 2 1865 0 4 100 99,78 3 2084 0 1 100 99,95 4 2229 1 17 99,95 99,24 5 2572 0 38 100 98,54 6 2532 1 2 99,96 99,92 7 2124 1 1 99,95 99,95 8 2539 1 1 99,96 99,96 9 1795 2 67 100 96,4 10 1879 2 20 99,89 98,94 Total tape 21892 8 151 99,97 99,26
The FN values are very low (range 0÷2); this is mainly related to the capability of the proposed algorithm to correctly detect any QRS complex and to the negligible number of artefacts of the ECG signal collected from the wearable
67
chest belt. Moreover, the ECG chest strap provided readable signal for more than 95% and 99% of the time of acquisition while the subjects were working and lying supine at bedside respectively. These results show the good performance of the ECG chest strap, in according to a gold standard, like the ELA Holter. The System has been used within an European project (CHIRON) where a lot of ECG data have been collected (in an Italian Server), at the moment:
• 523 files
• 50 Healthy • 473 Patients
The Patients are elderly people, with an high cardiovascular risk, they are been selected by a group of clinicians. I took a statistical sample (50 Healthy,100 Patients) and I extracted some features from this large amount of data.
Table 5. Results obtained from a features extraction (standard deviation of each features inside brackets)
68
It is important to put attention to RMSSD feature, that has the following equation:
𝑀𝑆𝑆𝐷 √
−
∑(
−
)
Figure 35. It shows the comparison of RMSSD between the Control group and the Patients
The behaviour of this feature seems to be like a marker, it is able to help the medical doctor to discriminate a pathological situation. It’s easy to see that this is a time domain feature and the algorithm to extract it doesn’t need much computational power, for this reason it’s possible to have a future development, that means the use of this important feature like a marker. The RMSSD extraction could be included directly inside the sensor that can monitor in real time the conditions of elderly people in order to do an efficient screening solving the problems previously described, about the absence of elderly person’s attitudes to use technologies.
69
3.7 Conclusions
I have collaborated for the development of a novel architecture, that combine three different layers, from Sensor to Server passing through the Mobile, in order to have a full monitoring of the patient’s clinical situation. In particular I faced some problems to put the elderly people able to use technologies (I found it within an European project) and I tried to solve this aspect with a migration strategy that consists to transfer the knowledge from the Server to the Sensor in order to obtain a clever system that is basically based by the use of only one device. The first step has been the investigation about the feasibility to make it, infact the important thing was to find a particular feature, like a marker, to discriminate a particular patient’s pathological case. This marker need to be easy to be found, by a computational point of view, because the sensor device has not a big power. As it’s possible to see in the results there is a feature, the RMSSD, that gives us the possibility to discriminate the cardiovascular state of high risk, for this reason I thought that it’s possible to migrate this information to sensor side, just to simplify all the architecture, still keeping the functionality.
70
Chapter 4 Recognition of
Elementary Upper Limb
Movements
4.1 Introduction
Motion tracking of human body parts has been applied in a wide range of applications such as remote health monitoring, human computer interaction and sports training using different sensing technologies like mechanical tracking, optical systems, acoustic tracking, radar systems and inertial/magnetic systems [21]. Advances in Wireless Sensor Networks (WSN) and Information and Communication Technology (ICT) have played a key role in the miniaturization of low-cost, body-worn, inertial sensors comprising of accelerometers, rate gyroscopes and magnetometers that are capable of capturing kinematic data [21] [22] to be used over a wide scale. The information extracted from such data has been used to compute joint angles, estimate orientation and for developing the kinematic model of the human body [23] which in effect helps to produce a quantitative measure of a physical activity or a qualitative measure such as the recognition of the type of activity, depending on the application area [24] [25]. An ageing population and an
71
increase in associated healthcare costs, specifically related to the treatment of chronic arthritis, cardiovascular or neurodegenerative diseases, have prompted an interest in telemedicine based systems enabling home-based rehabilitation [25] [26] [27]. Wireless monitoring of orientations of various body segments and joints is also being extensively used in a wide range of analysis prevalent in sporting activities [28]. Furthermore wireless sensing networks body area networks (WBANs) form a core part of ubiquitous computing and in particular, are being developed as controllers for intelligent social user interfaces (ISUIs) [29] [30]. The nonintrusive nature of wearable inertial sensors coupled with the advantages of wireless communication has made them an integral part of many such applications. In such wearable systems, the data analysis primarily needs to be carried out at the sensor node yielding energy efficient solutions as compared to conventional remote monitoring approaches based on continuous transmission of vital data. Hence, from the long-term system operation perspective, when implementing a wireless body area network that comprises a number of various sensors, it is imperative to select data analysis algorithms that are computationally of low complexity. Energy consumption being directly proportional to the computational complexity of the processing algorithm used, high-complexity algorithms (although they may be more ‘accurate’) will drain the battery faster, defying the objective of long-term monitoring. In my work I describe a systematic exploration to recognize three fundamental movements of the upper limb, generally associated with basic activities of daily living, using data collected from tri-axial accelerometers attached to the wrist. The three movements investigated, along with examples of their daily occurrence, were: extension/flexion of the forearm (reach out and retrieve object); rotation of